false
0001425205
0001425205
2024-01-08
2024-01-08
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
Current Report
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (date of earliest event reported): January 8, 2024
IOVANCE BIOTHERAPEUTICS, INC.
(Exact Name of Registrant as Specified in
Charter)
| Delaware |
| (State of Incorporation) |
| |
| 001-36860 |
|
75-3254381 |
| Commission File Number |
|
(I.R.S. Employer Identification No.) |
| |
|
|
| 825
Industrial Road, Suite 400 |
|
|
| San Carlos, California |
|
94070 |
| (Address of Principal Executive Offices) |
|
(Zip Code) |
| |
|
|
| (650) 260-7120 |
| (Registrant’s Telephone Number, Including Area Code) |
| |
Check the appropriate box below if the Form 8-K filing is intended
to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
|
¨ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425). |
|
¨ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12). |
|
¨ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)). |
|
¨ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)). |
Indicate
by check mark whether the registrant is an emerging growth company as defined in as defined in Rule 405 of the Securities Act
of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ¨
If
an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for
complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
Trading
Symbol(s) |
Name of each exchange on which
registered |
| Common stock, par value $0.000041666 per value |
IOVA |
The Nasdaq Stock Market, LLC |
On January 8, 2024, Iovance Biotherapeutics, Inc.
(the “Company”) updated its corporate presentation that it uses for presentations at healthcare conferences and to analysts,
current stockholders, and others. A copy of the Company’s presentation that it intends to use at such events, including the J.P. Morgan Healthcare Conference, is attached as Exhibit
99.1 and incorporated herein by reference.
| Item 9.01 |
Financial Statements and Exhibits. |
(d) Exhibits.
SIGNATURES
Pursuant to the requirements
of the Securities Exchange Act of 1934, the Registrant has duly caused this Report to be signed on its behalf by the undersigned hereunto
duly authorized.
| Date: January 8, 2024 |
IOVANCE BIOTHERAPEUTICS, INC. |
| |
|
|
| |
|
|
| |
By: |
/s/ Frederick G. Vogt |
| |
|
Frederick G. Vogt, Interim CEO & General Counsel |
Exhibit 99.1

1 © 2024, Iovance Biotherapeutics, Inc. © 2024, Iovance Biotherapeutics, Inc. Corporate Overview January 2024 1
2 © 2024, Iovance Biotherapeutics, Inc. Forward - Looking Statements Certain matters discussed in this press release are “forward - looking statements” of Iovance Biotherapeutics, Inc. (hereinafter r eferred to as the “Company,” “we,” “us,” or “our”) within the meaning of the Private Securities Litigation Reform Act of 1995 (the “PSLRA”). All such written or oral statements ma de in this press release, other than statements of historical fact, are forward - looking statements and are intended to be covered by the safe harbor for forward - looking statements provided by the PSLRA. Without limiting the foregoing, we may, in some cases, use terms such as “predicts,” “believes,” “potential,” “continue,” “estimates,” “anticipate s,” “expects,” “plans,” “intends,” “forecast,” “guidance,” “outlook,” “may,” “could,” “might,” “will,” “should” or other words that convey uncertainty of future events or o utc omes and are intended to identify forward - looking statements. Forward - looking statements are based on assumptions and assessments made in light of management’s experience and per ception of historical trends, current conditions, expected future developments and other factors believed to be appropriate. Forward - looking statements in this press release are made as of the date of this press release, and we undertake no duty to update or revise any such statements, whether as a result of new information, future eve nts or otherwise. Forward - looking statements are not guarantees of future performance and are subject to risks, uncertainties and other factors, many of which are outside of our control, that may cause actual results, levels of activity, performance, achievements and developments to be materially different from those expressed in or implied by these f orw ard - looking statements. Important factors that could cause actual results, developments and business decisions to differ materially from forward - looking statements are describ ed in the sections titled "Risk Factors" in our filings with the Securities and Exchange Commission, including our most recent Annual Report on Form 10 - K and Quarterly Reports on Form 10 - Q, and include, but are not limited to, the following substantial known and unknown risks and uncertainties inherent in our business: the effects of the COV ID - 19 pandemic; risks related to the timing of and our ability to successfully develop, submit, obtain, or maintain U.S. Food and Drug Administration (“FDA”), European Medicine s A gency (“EMA”), or other regulatory authority approval of, or other action with respect to, our product candidates, and our ability to successfully commercialize any produ ct candidates for which we obtain FDA, EMA, or other regulatory authority approval; whether clinical trial results from our pivotal studies and cohorts, and meetings with the FDA , E MA, or other regulatory authorities may support registrational studies and subsequent approvals by the FDA, EMA, or other regulatory authorities, including the risk that the pl anned single arm Phase 2 IOV - LUN - 202 trial may not support registration; preliminary and interim clinical results, which may include efficacy and safety results, from ongoing c lin ical trials or cohorts may not be reflected in the final analyses of our ongoing clinical trials or subgroups within these trials or in other prior trials or cohorts; the risk that e nro llment may need to be adjusted for our trials and cohorts within those trials based on FDA and other regulatory agency input; the risk that the changing landscape of care for cervical ca ncer patients may impact our clinical trials in this indication; the risk that we may be required to conduct additional clinical trials or modify ongoing or future clinical trial s b ased on feedback from the FDA, EMA, or other regulatory authorities; the risk that our interpretation of the results of our clinical trials or communications with the FDA, EMA, or o the r regulatory authorities may differ from the interpretation of such results or communications by such regulatory authorities (including from the prior pre - BLA meeting with t he FDA and/or regarding our prior meetings with the FDA regarding our NSCLC clinical trials); the risk that the FDA, EMA, or other regulatory authorities may not approve or may delay approval for our BLA submission for lifileucel in metastatic melanoma; the acceptance by the market of our product candidates and their potential reimbursement by payors, i f a pproved, in the U.S. and other international markets; our ability or inability to manufacture our therapies using third party manufacturers or our own facility may advers ely affect our potential commercial launch; the results of clinical trials with collaborators using different manufacturing processes may not be reflected in our sponsored trials; t he risk regarding the successful integration of the recent Proleukin acquisition; the risk that the successful development or commercialization of our products may not generate suffici ent revenue from product sales, and we may not become profitable in the near term, or at all; the risk that unanticipated expenses may decrease our estimated cash balances and forecasts and increase our estimated capital requirements; and other factors, including general economic conditions and regulatory developments, not within our control.
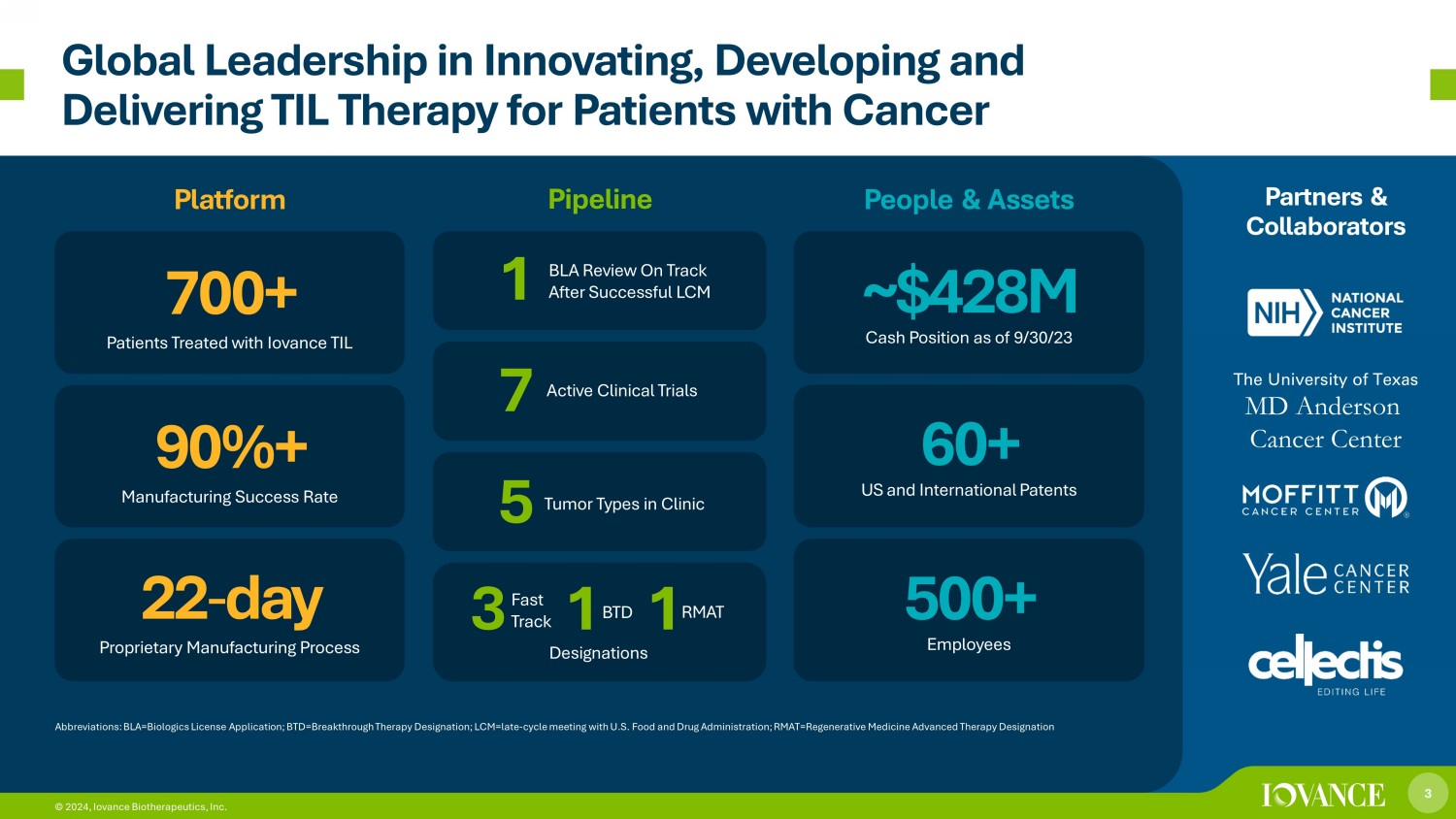
3 © 2024, Iovance Biotherapeutics, Inc. Global Leadership in Innovating, Developing and Delivering TIL Therapy for Patients with Cancer Platform Pipeline People & Assets Partners & Collaborators Abbreviations: BLA=Biologics License Application; BTD=Breakthrough Therapy Designation; LCM=late - cycle meeting with U.S. Food and Drug Administration; RMAT =Regenerative Medicine Advanced Therapy Designation 22 - day Proprietary Manufacturing Process 90%+ Manufacturing Success Rate 7 00+ Patients Treated with Iovance TIL ~$ 428 M Cash Position as of 9/30/23 60+ US and International Patents 500+ Employees The University of Texas MD Anderson Cancer Center 3 © 2024, Iovance Biotherapeutics, Inc. 3 1 1 Designations Active Clinical Trials 7 Tumor Types in Clinic 5 BLA Review On Track After Successful LCM Fast Track BTD RMAT 1
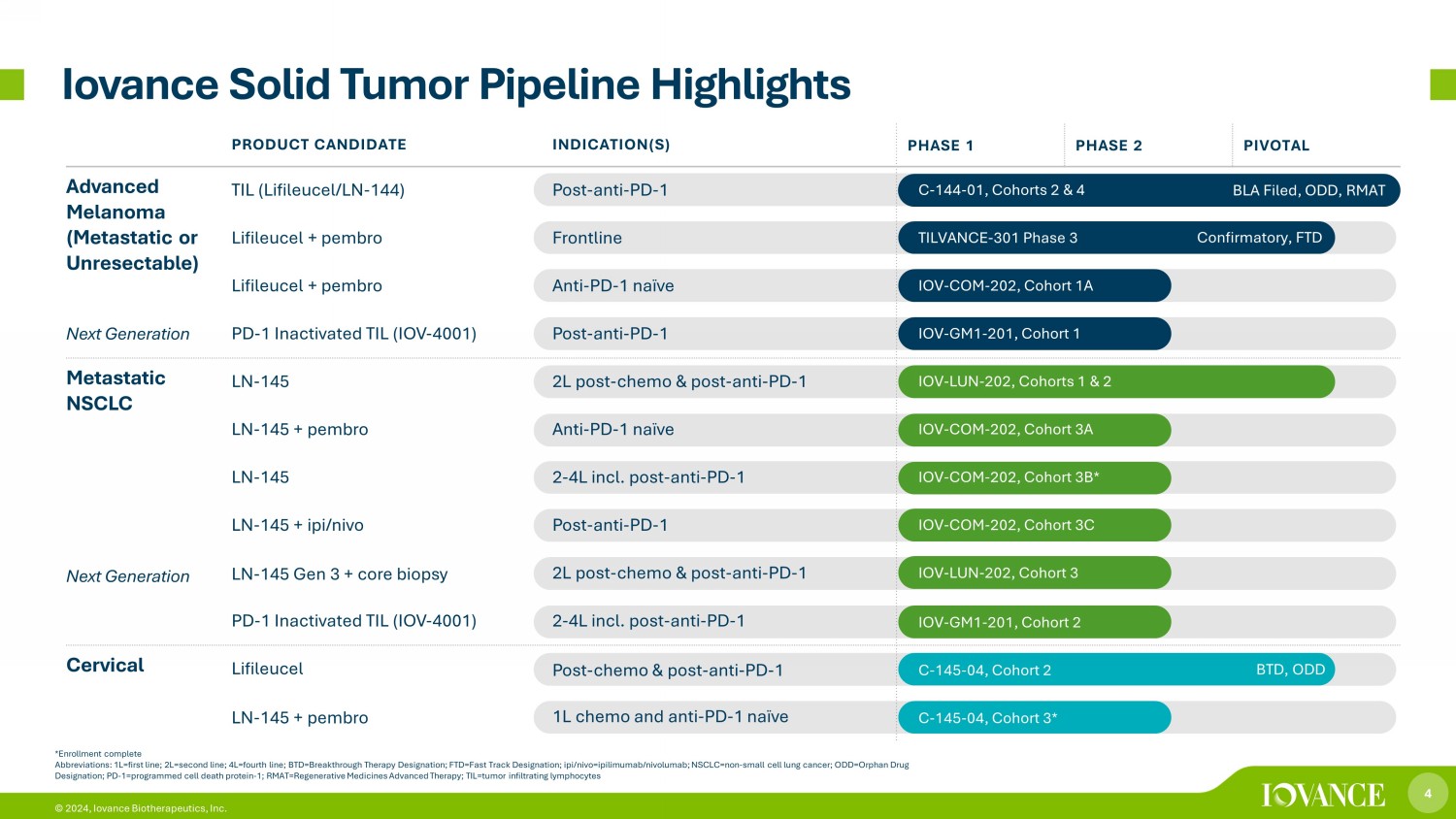
4 © 2024, Iovance Biotherapeutics, Inc. *Enrollment complete Abbreviations: 1L=first line; 2L=second line; 4L=fourth line; BTD=Breakthrough Therapy Designation; FTD=Fast Track Designatio n; ipi/nivo=ipilimumab/nivolumab; NSCLC=non - small cell lung cancer; ODD=Orphan Drug Designation; PD - 1=programmed cell death protein - 1; RMAT=Regenerative Medicines Advanced Therapy; TIL=tumor infiltrating lymphocy tes Iovance Solid Tumor Pipeline Highlights Confirmatory, FTD BLA Filed, ODD, RMAT BTD, ODD PRODUCT CANDIDATE INDICATION(S) PHASE 1 PHASE 2 PIVOTAL Advanced Melanoma (Metastatic or Unresectable) Next Generation TIL (Lifileucel/LN - 144) Post - anti - PD - 1 C - 144 - 01, Cohorts 2 & 4 Lifileucel + pembro Frontline TILVANCE - 301 Phase 3 Lifileucel + pembro Anti - PD - 1 naïve IOV - COM - 202, Cohort 1A PD - 1 Inactivated TIL (IOV - 4001) Post - anti - PD - 1 IOV - GM1 - 201, Cohort 1 Metastatic NSCLC Next Generation LN - 145 2L post - chemo & post - anti - PD - 1 IOV - LUN - 202, Cohorts 1 & 2 LN - 145 + pembro Anti - PD - 1 naïve IOV - COM - 202, Cohort 3A LN - 145 2 - 4L incl. post - anti - PD - 1 IOV - COM - 202, Cohort 3B* LN - 145 + ipi/nivo Post - anti - PD - 1 IOV - COM - 202, Cohort 3C LN - 145 Gen 3 + core biopsy 2L post - chemo & post - anti - PD - 1 IOV - LUN - 202, Cohort 3 PD - 1 Inactivated TIL (IOV - 4001) 2 - 4L incl. post - anti - PD - 1 IOV - GM1 - 201, Cohort 2 Cervical Lifileucel Post - chemo & post - anti - PD - 1 C - 145 - 04, Cohort 2 LN - 145 + pembro 1L chemo and anti - PD - 1 naïve C - 145 - 04, Cohort 3*
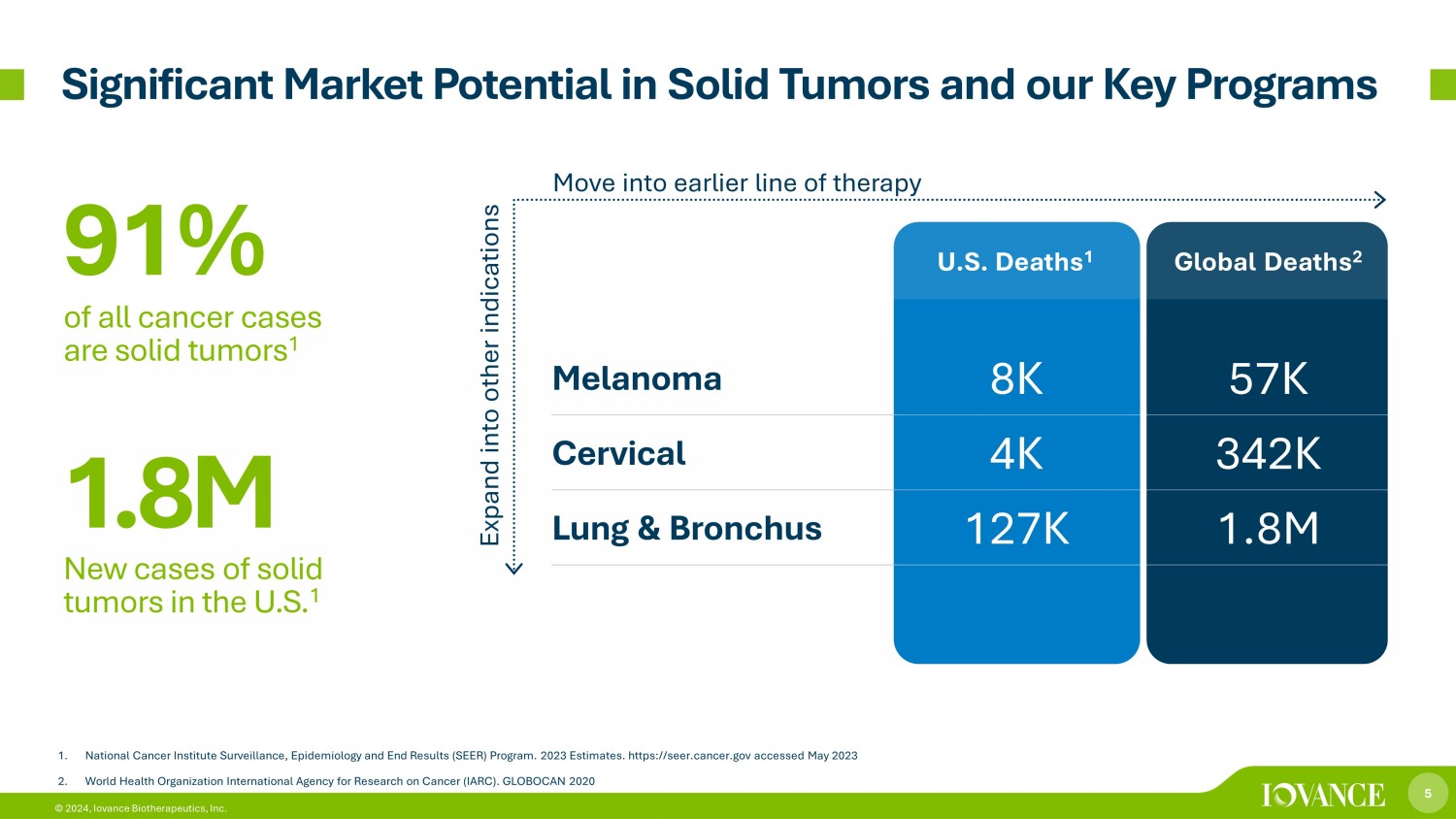
5 © 2024, Iovance Biotherapeutics, Inc. 1. National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program. 2023 Estimates. https://seer.cancer.gov acc essed May 2023 2. World Health Organization International Agency for Research on Cancer (IARC). GLOBOCAN 2020 U.S. Deaths 1 Global Deaths 2 Melanoma 8K 57K Cervical 4K 342K Lung & Bronchus 127K 1.8M 91% of all cancer cases are solid tumors 1 1 .8 M New cases of solid tumors in the U.S. 1 Expand into other indications Move into earlier line of therapy Significant Market Potential in Solid Tumors and our Key Programs
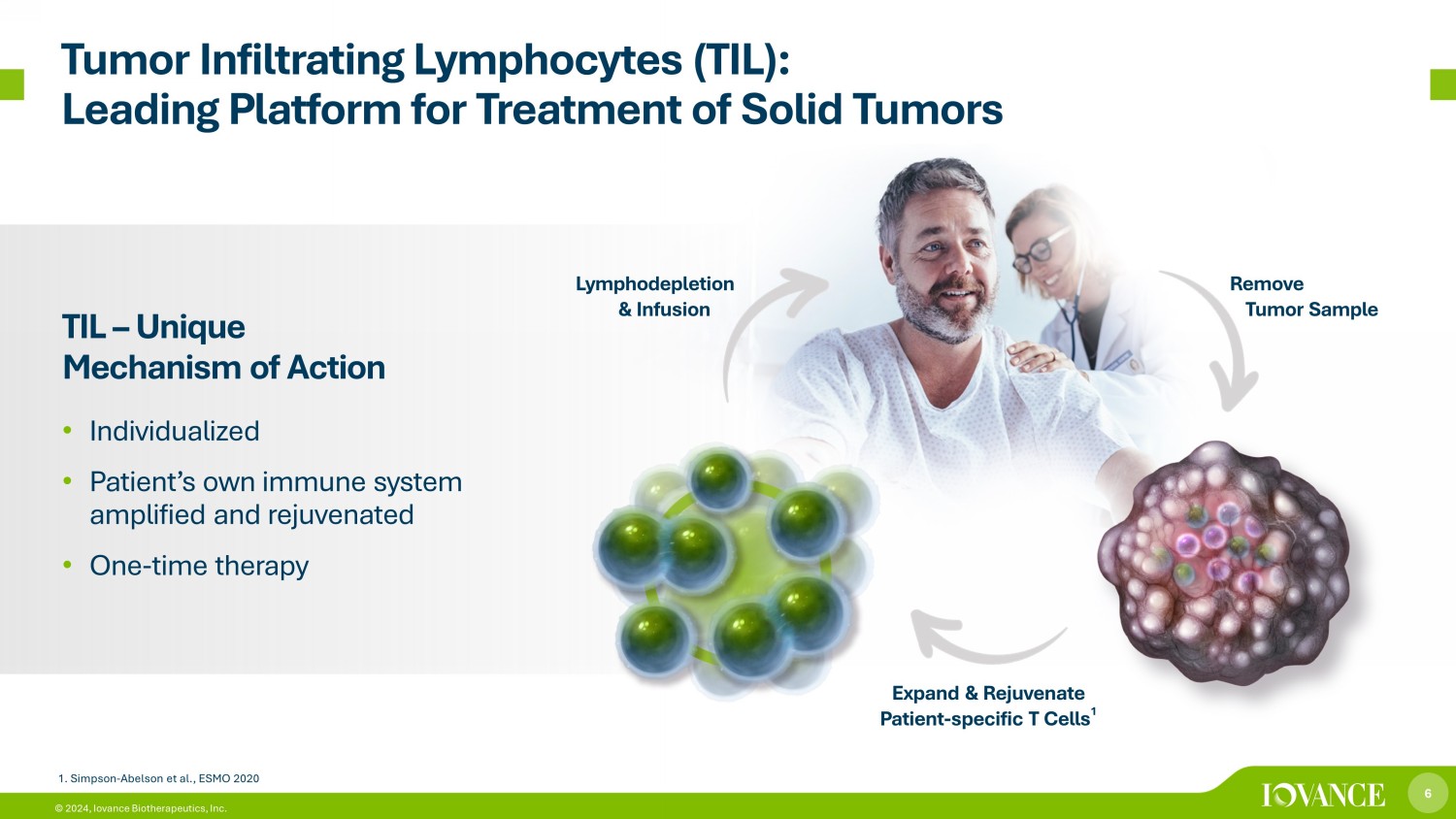
6 © 2024, Iovance Biotherapeutics, Inc. Tumor Infiltrating Lymphocytes (TIL): Leading Platform for Treatment of Solid Tumors TIL – Unique Mechanism of Action • Individualized • Patient’s own immune system amplified and rejuvenated • One - time therapy Remove Tumor Sample Expand & Rejuvenate Patient - specific T Cells 1 Lymphodepletion & Infusion 1. Simpson - Abelson et al., ESMO 2020

7 © 2024, Iovance Biotherapeutics, Inc. Tumor TIL Mechanism of Action TIL Peripheral blood Blood vessel Tumor cell TIL TIL Tumor bed TIL Lysing tumor cell T - cell receptor Tumor neoantigen peptides MHC - I/II Chemokine receptor Circulation Migration Peptide Antigen Recognition Lysis (Tumor Killing) Chemokine TIL IFN Granzyme Perforin TIL Iovance TIL therapy deploys billions of individualized patient - specific polyclonal TIL cells to recognize and target a multitude of non - overlapping neoantigens in patients with solid tumors Lysing tumor cell

8 © 2024, Iovance Biotherapeutics, Inc. Iovance Streamlined 22 - Day GMP Manufacturing Process 1 2 Patient Intake Tumor Sample Procurement 3 4 NMA - LD TIL 5 6 IL - 2 Recovery/Discharge 4 2 Gen 2 Process: 22 Days 8 © 2024, Iovance Biotherapeutics, Inc. Abbreviations: GMP= good manufacturing practice; IL - 2=interleukin - 2; NMA - LD=nonmyeloablative lymphodepletion

9 © 2024, Iovance Biotherapeutics, Inc. Iovance Cell Therapy Center: i CTC Built - to - suit custom facility in Navy Yard Philadelphia 136,000 ft 2 , $85M investment LEED gold certification for core and shell building Clinical supply initiated 3Q21 Successfully completed FDA Pre - License Inspection in 2023 Commercial manufacturing expected with BLA approval Control to optimize capacity, quality & COGS Leading Cell Therapy Manufacturing Facility
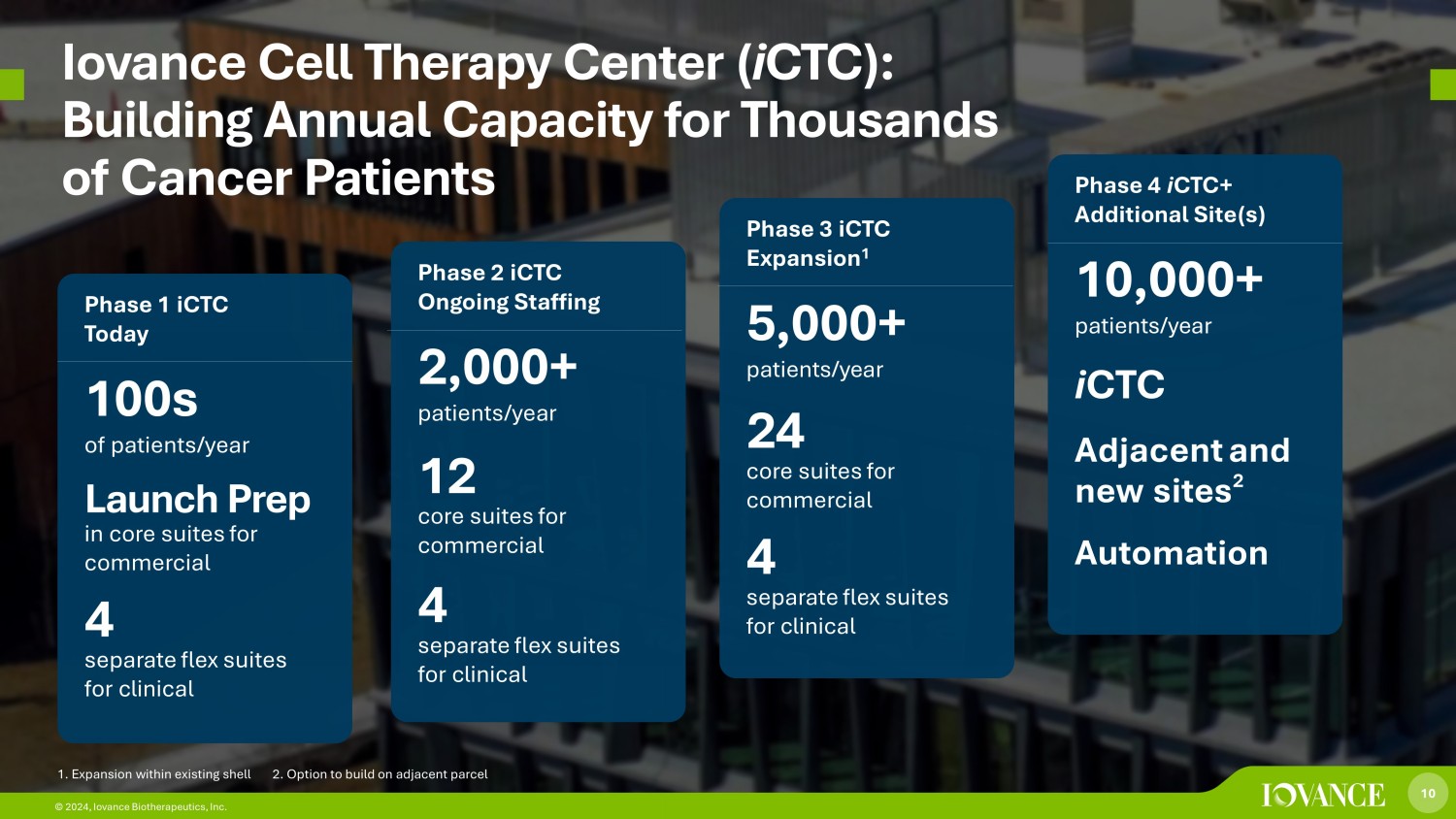
10 © 2024, Iovance Biotherapeutics, Inc. Iovance Cell Therapy Center ( i CTC): Building Annual Capacity for Thousands of Cancer Patients Phase 1 iCTC Today 100s of patients/year Launch Prep in core suites for commercial 4 separate flex suites for clinical Phase 2 iCTC Ongoing Staffing 2,000+ patients/year 12 core suites for commercial 4 separate flex suites for clinical Phase 3 iCTC Expansion 1 5,000+ patients/year 24 core suites for commercial 4 separate flex suites for clinical Phase 4 i CTC+ Additional Site(s) 10,000+ patients/year i CTC Adjacent and new sites 2 Automation 10 © 2024, Iovance Biotherapeutics, Inc. 1. Expansion within existing shell 2. Option to build on adjacent parcel
11 © 2024, Iovance Biotherapeutics, Inc. 11 Iovance TIL Therapy in Advanced Melanoma

12 © 2024, Iovance Biotherapeutics, Inc. U.S. Unmet Medical Need for Metastatic Melanoma Therapy No FDA Approved Treatment Options After Progression on ICI (Anti - PD - 1) Therapy and BRAF/MEK inhibitors BRAF/MEK inhibitors if BRAF mutation + Chemotherapy ORR 4 - 10% 5 mOS ~7 - 8 months 6 Anti - PD - 1 Immunotherapy 21% - 33% ORR 4 Available Care: 9.9K 6.3K 4.8K 1L 2L 3L-4L Melanoma Drug - Treated Population in 2021 3 Unresectable / Metastatic (US) 1L 2L+ Abbreviations: 1L=first line therapy, 2L=second line therapy, 3L=third line therapy, 4L=fourth line therapy; ICI=immune check poi nt inhibitor; ORR=objective response rate; mOS=median overall survival; PD - 1=programmed cell death protein - 1 15k Annual new cases of advanced melanoma in U.S. 1 8k Annual deaths in U.S. 2 1. Estimate of US incidence (2021) of unresectable or metastatic melanoma based on secondary and primary market research 2. National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program. 2023 Estimates. https://seer.cancer.gov accessed May 2023 3. Clarivate DRG Disease Landscape (2021) 4. Keytruda USPI 5. Keytruda USPI (4%) and Weber et al., Lancet Oncol 2015 (ICC 10%) 6. Kirchburger et al., Eur J Cancer 2016 and Goldinger et al., J Clin Oncol 2018
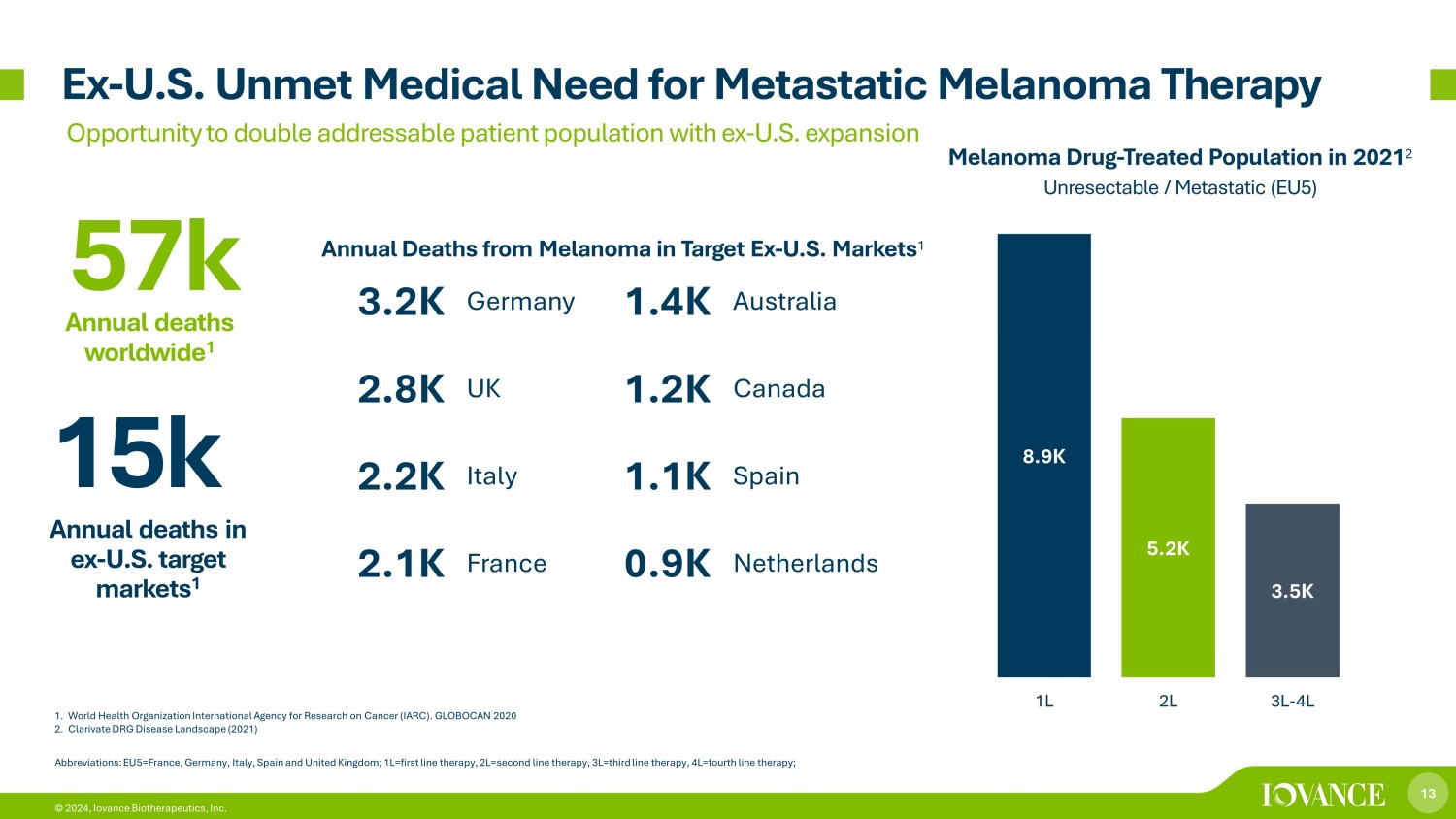
13 © 2024, Iovance Biotherapeutics, Inc. 1. World Health Organization International Agency for Research on Cancer (IARC). GLOBOCAN 2020 2. Clarivate DRG Disease Landscape (2021) Ex - U.S. Unmet Medical Need for Metastatic Melanoma Therapy Opportunity to double addressable patient population with ex - U.S. expansion 8.9K 5.2K 3.5K 1L 2L 3L-4L Melanoma Drug - Treated Population in 2021 2 Unresectable / Metastatic (EU5) Abbreviations: EU5=France, Germany, Italy, Spain and United Kingdom; 1L=first line therapy, 2L=second line therapy, 3L=third lin e therapy, 4L=fourth line therapy; 15k Annual deaths in ex - U.S. target markets 1 3.2K Germany 1.4K Australia 2.8K UK 1.2K Canada 2.2K Italy 1.1K Spain 2.1K France 0.9K Netherlands 57k Annual deaths worldwide 1 Annual Deaths from Melanoma in Target Ex - U.S. Markets 1
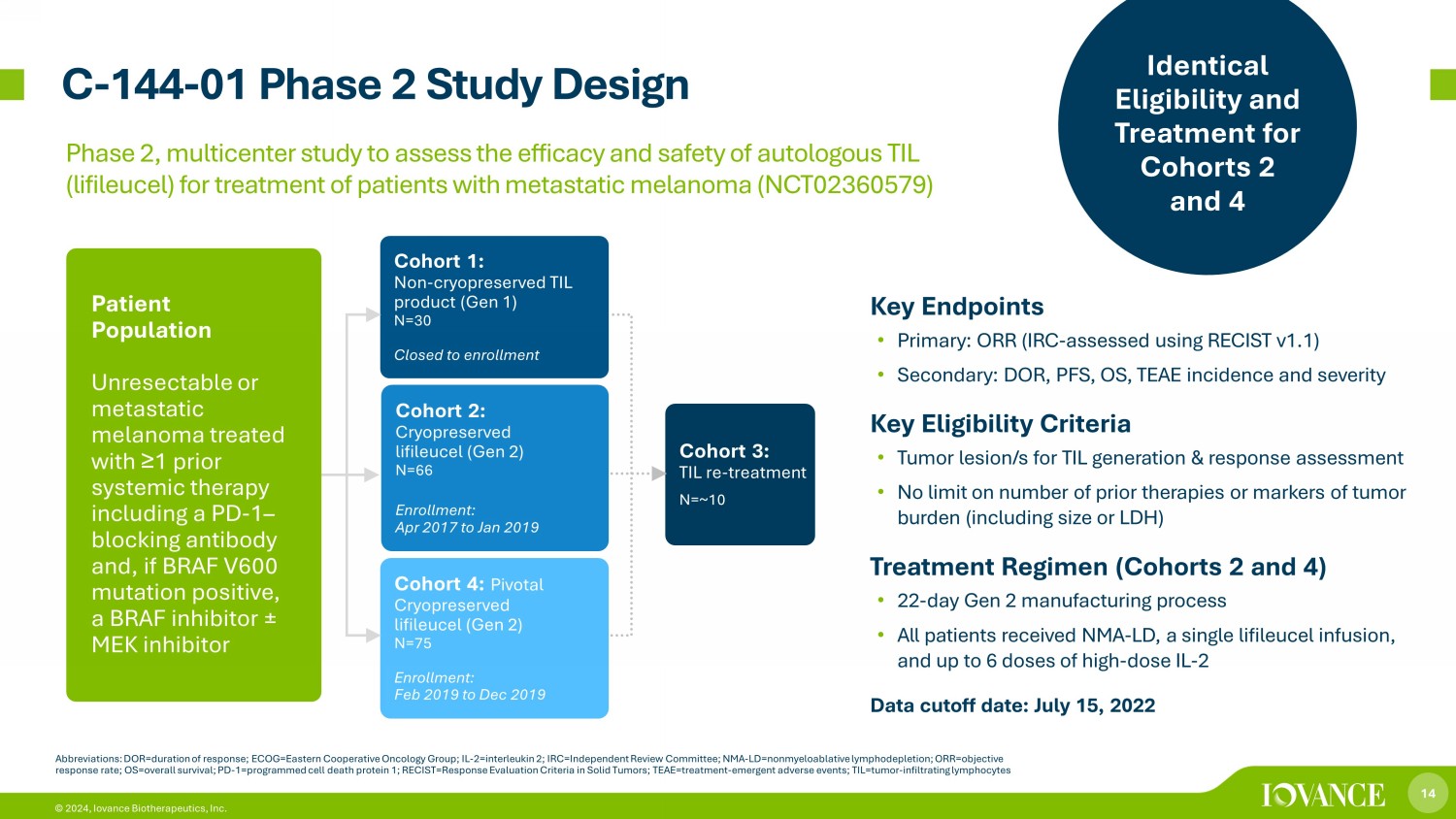
14 © 2024, Iovance Biotherapeutics, Inc. C - 144 - 01 Phase 2 Study Design Abbreviations: DOR=duration of response; ECOG=Eastern Cooperative Oncology Group; IL - 2=interleukin 2; IRC=Independent Review Committee; NMA - LD= nonmyeloablative lymphodepletion; ORR=objective response rate; OS=overall survival; PD - 1=programmed cell death protein 1; RECIST=Response Evaluation Criteria in Solid Tumors; T EAE=treatment - emergent adverse events; TIL=tumor - infiltrating lymphocytes Cohort 1: Non - cryopreserved TIL product (Gen 1) N=30 Closed to enrollment Cohort 2: Cryopreserved lifileucel (Gen 2) N=66 Enrollment: Apr 2017 to Jan 2019 Cohort 3: TIL re - treatment N=~10 Patient Population Unresectable or metastatic melanoma treated with ≥ 1 prior systemic therapy including a PD - 1 – blocking antibody and, if BRAF V600 mutation positive, a BRAF inhibitor ± MEK inhibitor Cohort 4: Pivotal Cryopreserved lifileucel (Gen 2) N=75 Enrollment: Feb 2019 to Dec 2019 Key Endpoints • Primary: ORR (IRC - assessed using RECIST v1.1) • Secondary: DOR, PFS, OS, TEAE incidence and severity Key Eligibility Criteria • Tumor lesion/s for TIL generation & response assessment • No limit on number of prior therapies or markers of tumor burden (including size or LDH) Treatment Regimen (Cohorts 2 and 4) • 22 - day Gen 2 manufacturing process • All patients received NMA - LD, a single lifileucel infusion, and up to 6 doses of high - dose IL - 2 Data cutoff date: July 15, 2022 Identical Eligibility and Treatment for Cohorts 2 and 4 Phase 2, multicenter study to assess the efficacy and safety of autologous TIL (lifileucel) for treatment of patients with metastatic melanoma (NCT02360579)
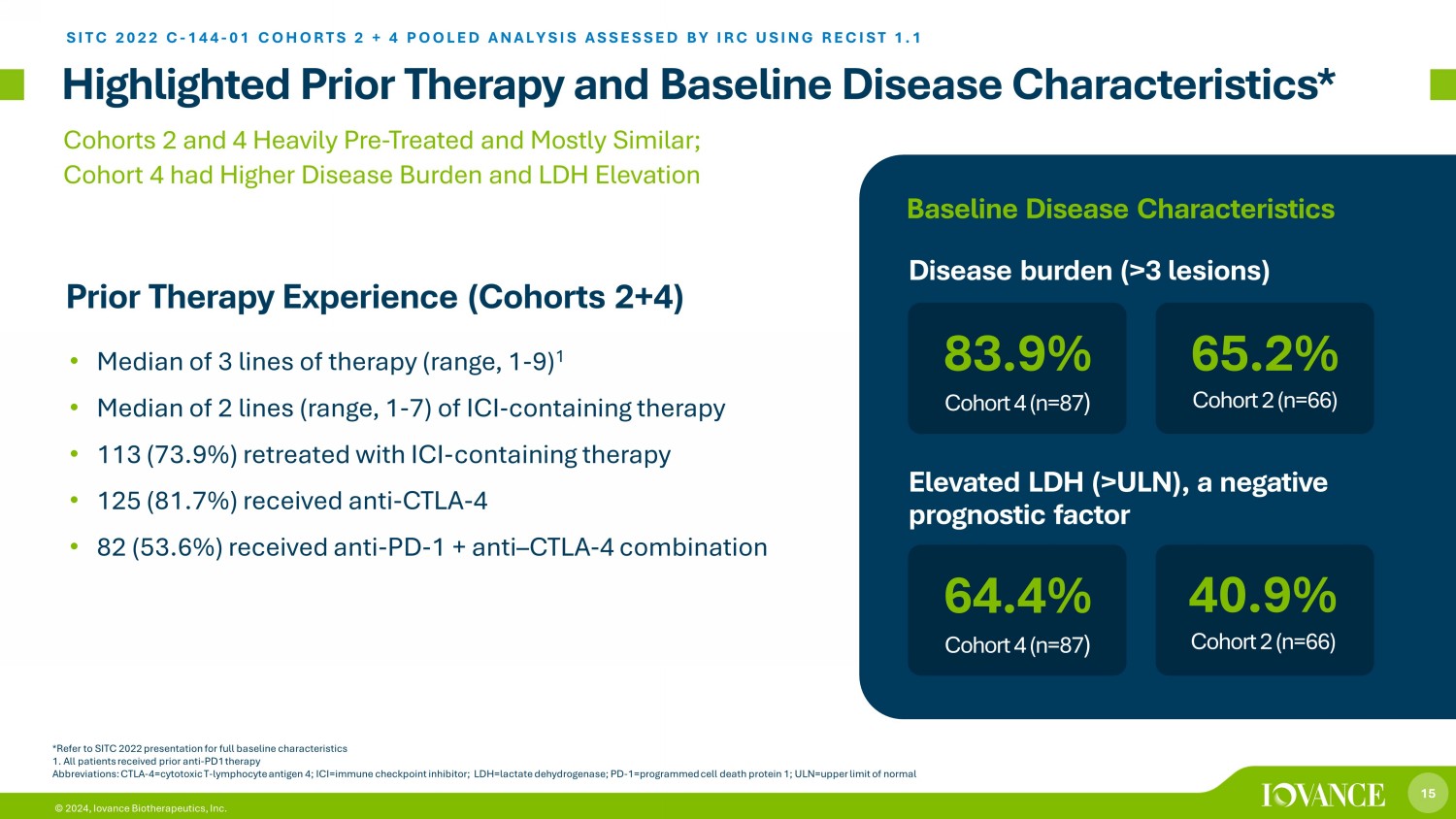
15 © 2024, Iovance Biotherapeutics, Inc. Highlighted Prior Therapy and Baseline Disease Characteristics* *Refer to SITC 2022 presentation for full baseline characteristics 1. All patients received prior anti - PD1 therapy Abbreviations: CTLA - 4=cytotoxic T - lymphocyte antigen 4; ICI=immune checkpoint inhibitor; LDH=lactate dehydrogenase; PD - 1=progra mmed cell death protein 1; ULN=upper limit of normal • Median of 3 lines of therapy (range, 1 - 9) 1 • Median of 2 lines (range, 1 - 7) of ICI - containing therapy • 113 (73.9%) retreated with ICI - containing therapy • 125 (81.7%) received anti - CTLA - 4 • 82 (53.6%) received anti - PD - 1 + anti – CTLA - 4 combination Cohorts 2 and 4 Heavily Pre - Treated and Mostly Similar; Cohort 4 had Higher Disease Burden and LDH Elevation Prior Therapy Experience (Cohorts 2+4) SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 64.4% Cohort 4 (n=87 ) Disease burden (>3 lesions) 40.9% Cohort 2 (n=66) 83.9% Cohort 4 (n=87 ) 65.2% Cohort 2 (n=66) Elevated LDH (>ULN), a negative prognostic factor Baseline Disease Characteristics

16 © 2024, Iovance Biotherapeutics, Inc. Safety Non - Hematologic TEAEs in ≥ 30% of Patients* , † *Per CTCAE v4.03; Safety Analysis Set (N=156). † Grade 5 TEAEs included pneumonia (n=1), acute respiratory failure (n=1), arrhythmia (n=1), and intra - abdominal hemorrhage (n=1). All occurrences of AEs were counted if a patient experienced a new onset of the same AE at different timepoints. If multiple rec ords were reported on the electronic case report form because of toxicity grade decrease of the same AE that had not resolved, then the event was counted once with the highest grade reported.15 events were reported after Month 12 (Grade 1, n= 7; Grade 2, n=6; Grade 3, n=1; Grade 5, n=1) Abbreviations: AE=adverse event; D=day; IL - 2=interleukin 2; M, month; NMA - LD=nonmyeloablative lymphodepletion; TEAE=treatment - em ergent adverse event • Median of 6 IL - 2 doses administered • All patients experienced ≥ 1 TEAE (any grade); 94.9% experienced ≥ 1 Grade 3/4 TEAE • TEAEs were consistent with known safety profiles of NMA - LD and IL - 2 and in line with previous reports • Incidence of TEAEs decreased rapidly within the first 2 weeks after lifileucel infusion Preferred Term, n (%) Any Grade Grade 3/4 Chills 117 (75.0) 8 (5.1) Pyrexia 81 (51.9) 17 (10.9) Febrile neutropenia 65 (41.7) 65 (41.7) Hypophosphatemia 58 (37.2) 41 (26.3) Hypotension 52 (33.3) 17 (10.9) Fatigue 51 (32.7) 6 (3.8) Diarrhea 48 (30.8) 2 (1.3) Preferred Term, n (%) Grade 3/4 Leukopenia 156 (100.0) Lymphopenia 156 (100.0) Neutropenia 156 (100.0) Thrombocytopenia 147 (94.2) Anemia 111 (71.2) Grade 3/4 Hematologic Lab Abnormalities* *UDGH � � � � � SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 Transient and Manageable Nature of AEs Support the Potential Benefit of One - Time Treatment with Lifileucel

17 © 2024, Iovance Biotherapeutics, Inc. Objective Response Rate (ORR) of 31.4% by IRC SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 91% Concordance Rate between IRC - and Investigator - assessed ORR *Patient did not have acceptable target lesions and had best overall response of non - CR/non - PD per IRC assessment † Six patients were nonevaluable for response (5 due to early death; 1 due to new anticancer therapy) Abbreviations: CR,=complete response; IRC=independent review committee; ORR=objective response rate; PD=progressive disease; PR= partial response; SD=stable disease Cohort 2 (n=66) Cohort 4 (n=87) Cohort 2+4 (n=153) ORR, n (%) 23 (34.8) 25 (28.7) 48 (31.4) (95% CI) (23.5, 47.6) (19.5, 39.4) (24.1, 39.4) Best overall response, n (%) CR 5 (7.6) 4 (4.6) 9 (5.9) PR 18 (27.3) 21 (24.1) 39 (25.5) SD 24 (36.4) 47 (54.0) 71 (46.4) Non - CR/Non - PD* 1 (1.5) 0 1 (0.7) PD 15 (22.7) 12 (13.8) 27 (17.6) Nonevaluable † 3 (4.5) 3 (3.4) 6 (3.9) • 33 days median time from resection to lifileucel infusion • Lifileucel manufactured within specification in 94.7% of patients • Median number of TIL cells infused was 21.1 × 10 9 (range, 1.2 × 10 9 to 99.5 × 10 9 )
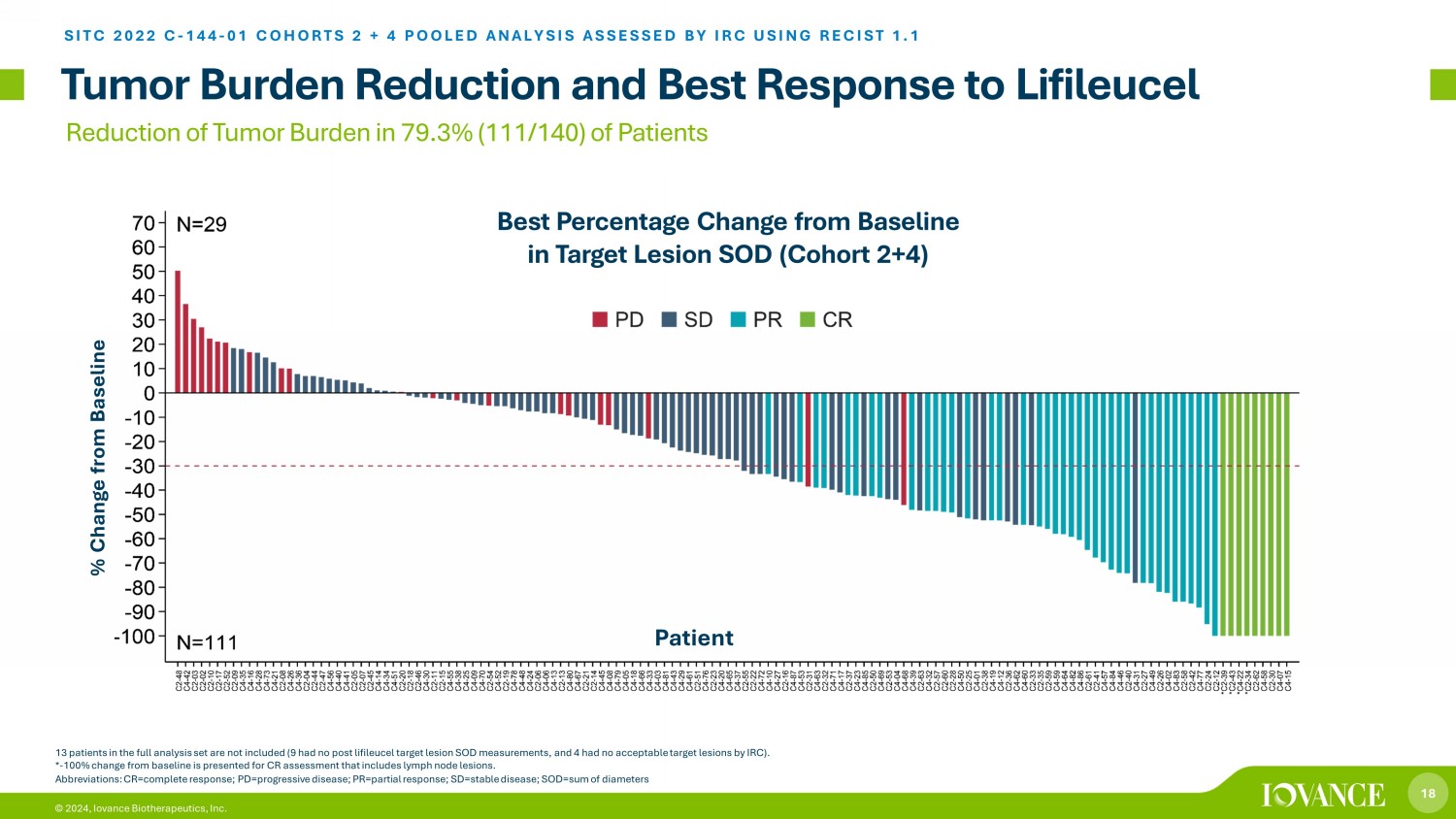
18 © 2024, Iovance Biotherapeutics, Inc. Tumor Burden Reduction and Best Response to Lifileucel SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 13 patients in the full analysis set are not included (9 had no post lifileucel target lesion SOD measurements, and 4 had no acc ep table target lesions by IRC). * - 100% change from baseline is presented for CR assessment that includes lymph node lesions. Best Percentage Change from Baseline in Target Lesion SOD (Cohort 2+4) Reduction of Tumor Burden in 79.3% (111/140) of Patients Abbreviations: CR=complete response; PD=progressive disease; PR=partial response; SD=stable disease; SOD=sum of diameters % Change from Baseline Patient
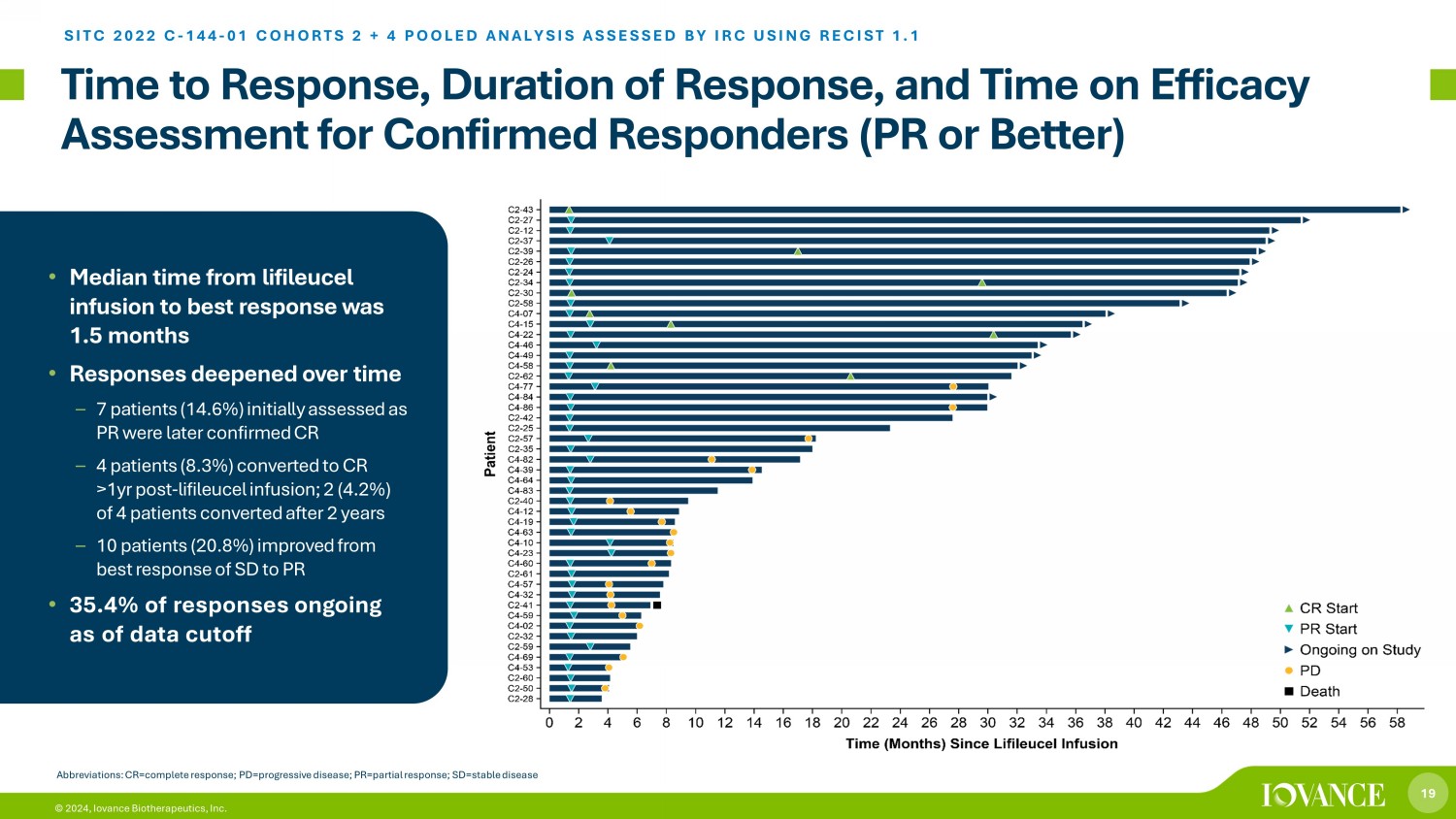
19 © 2024, Iovance Biotherapeutics, Inc. Time to Response, Duration of Response, and Time on Efficacy Assessment for Confirmed Responders (PR or Better) SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 • Median time from lifileucel infusion to best response was 1.5 months • Responses deepened over time – 7 patients (14.6%) initially assessed as PR were later confirmed CR – 4 patients (8.3%) converted to CR >1yr post - lifileucel infusion; 2 (4.2%) of 4 patients converted after 2 years – 10 patients (20.8%) improved from best response of SD to PR • 35.4% of responses ongoing as of data cutoff Abbreviations: CR=complete response; PD=progressive disease; PR=partial response; SD=stable disease
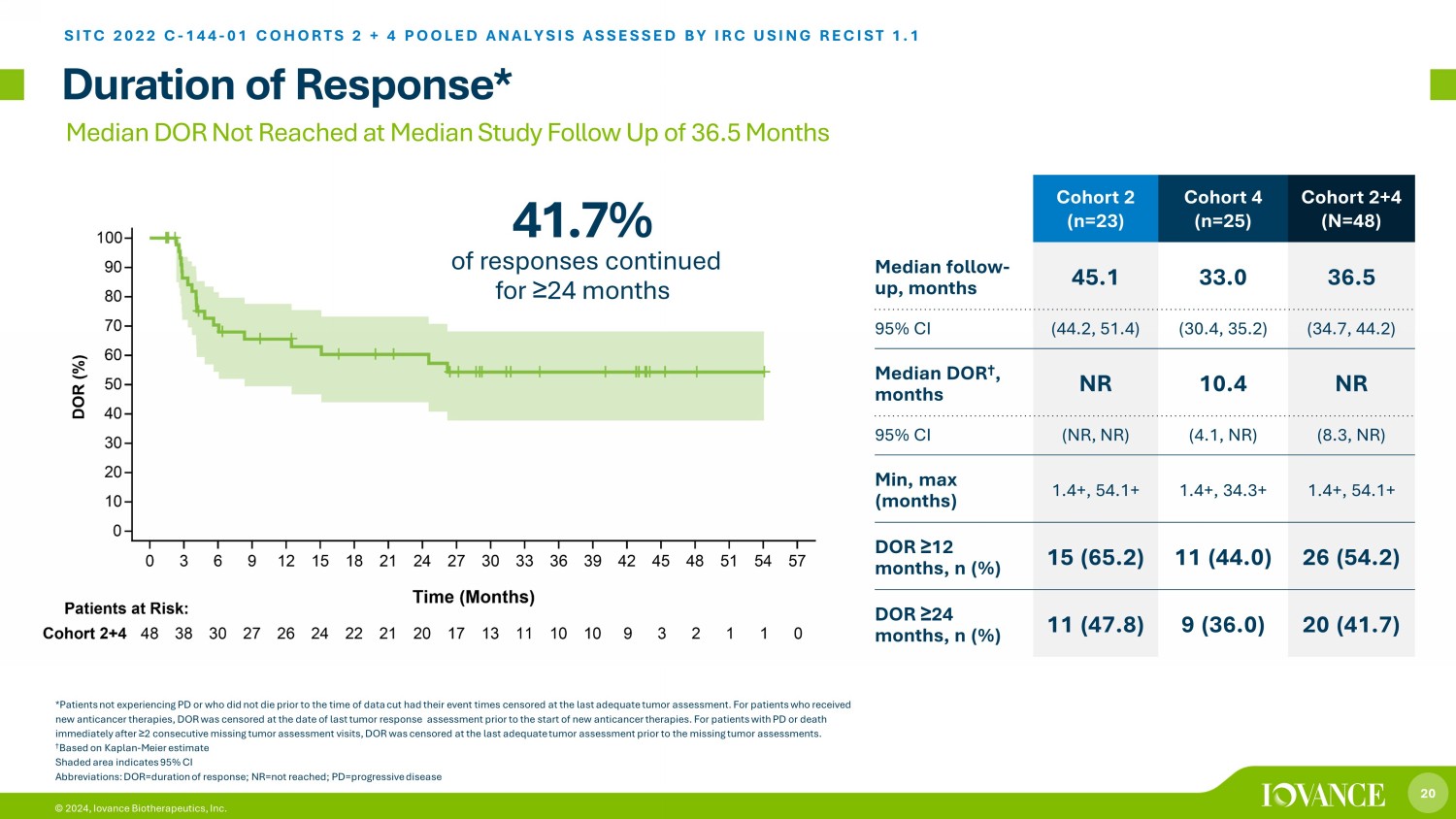
20 © 2024, Iovance Biotherapeutics, Inc. Cohort 2 (n=23) Cohort 4 (n=25) Cohort 2+4 (N=48) Median follow - up, months 45.1 33.0 36.5 95% CI (44.2, 51.4) (30.4, 35.2) (34.7, 44.2) Median DOR † , months NR 10.4 NR 95% CI (NR, NR) (4.1, NR) (8.3, NR) Min, max (months) 1.4+, 54.1+ 1.4+, 34.3+ 1.4+, 54.1+ DOR ≥ 12 months, n (%) 15 (65.2) 11 (44.0) 26 (54.2) DOR ≥ 24 months, n (%) 11 (47.8) 9 (36.0) 20 (41.7) Duration of Response* SITC 2022 C - 144 - 01 COHORTS 2 + 4 POOLED ANALYSIS ASSESSED BY IRC USING RECIST 1.1 *Patients not experiencing PD or who did not die prior to the time of data cut had their event times censored at the last ade qua te tumor assessment. For patients who received new anticancer therapies, DOR was censored at the date of last tumor response assessment prior to the start of new anticance r t herapies. For patients with PD or death immediately after ≥ 2 consecutive missing tumor assessment visits, DOR was censored at the last adequate tumor assessment prior to the missing tu mor assessments. † Based on Kaplan - Meier estimate Shaded area indicates 95% CI Abbreviations: DOR=duration of response; NR=not reached; PD=progressive disease Median DOR Not Reached at Median Study Follow Up of 36.5 Months 41.7% of responses continued for ≥ 24 months
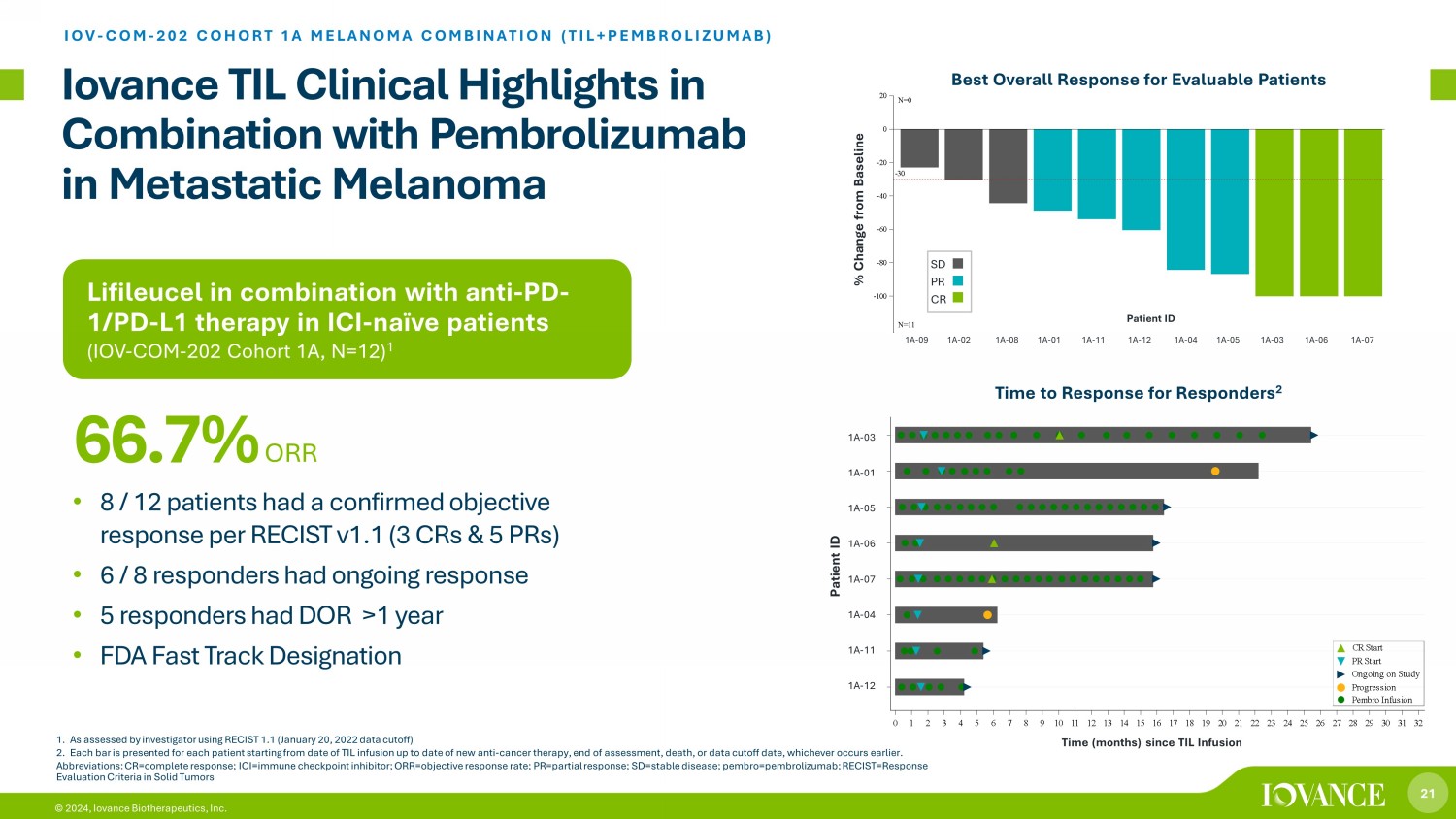
21 © 2024, Iovance Biotherapeutics, Inc. Lifileucel in combination with anti - PD - 1/PD - L1 therapy in ICI - naïve patients (IOV - COM - 202 Cohort 1A, N=12 ) 1 Iovance TIL Clinical Highlights in Combination with Pembrolizumab in Metastatic Melanoma IOV - COM - 202 COHORT 1A MELANOMA COMBINATION (TIL+PEMBROLIZUMAB) • 8 / 12 patients had a confirmed objective response per RECIST v1.1 (3 CRs & 5 PRs) • 6 / 8 responders had ongoing response • 5 responders had DOR >1 year • FDA Fast Track Designation 66.7% ORR 1. As assessed by investigator using RECIST 1.1 (January 20, 2022 data cutoff) 2. Each bar is presented for each patient starting from date of TIL infusion up to date of new anti - cancer therapy, end of assessme nt, death, or data cutoff date, whichever occurs earlier. Abbreviations: CR=complete response; ICI=immune checkpoint inhibitor; ORR=objective response rate; PR=partial response; SD=st abl e disease; pembro=pembrolizumab; RECIST=Response Evaluation Criteria in Solid Tumors Time (months) since TIL Infusion 1A-12 1A-11 1A-04 1A-07 1A-06 1A-05 1A-01 1A-03 S u b j e c t s 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 Time (months) since TIL Infusion Pembro Infusion Progression Ongoing on Study PR Start CR Start Time (months) since TIL Infusion 1A - 03 1A - 01 1A - 05 1A - 06 1A - 07 1A - 04 1A - 11 1A - 12 Patient ID Time to Response for Responders 2 Patient ID CRPRSD Best Overall Response -30 1A-09 1A-02 1A-08 1A-01 1A-11 1A-12 1A-04 1A-05 1A-03 1A-06 1A-07 -100 -80 -60 -40 -20 0 20 % C h a n g e f r o m B a s e l i n e N=0 N=11 Cohort 1A % Change from Baseline SD PR CR 1A - 09 1A - 02 1A - 08 1A - 01 1A - 11 1A - 12 1A - 04 1A - 05 1A - 03 1A - 06 1A - 07 Patient ID Best Overall Response for Evaluable Patients

22 © 2024, Iovance Biotherapeutics, Inc. 1:1 Randomization TILVANCE - 301 Global Phase 3 and Confirmatory Trial LIFILEUCEL + PEMBROLIZUMAB IN FRONTLINE ADVANCED MELANOMA Abbreviations: BIRC, blinded independent review committee; ORR=objective response rate; PD=progressive disease; PD - 1, programme d cell death protein - 1; PFS=progression free survival Arm A: lifileucel plus pembrolizumab Long - term follow up Patient Population Unresectable or metastatic melanoma; no prior therapy for metastatic disease N=670 Arm B: pembrolizumab alone Study Design with FDA Agreement • Dual Primary Endpoints: ORR & PFS • Registrational for frontline melanoma • Confirmatory for full approval in post - anti - PD - 1 melanoma • First patient randomized 2Q23 Option to crossover to lifileucel after BIRC - confirmed PD Randomized, multicenter study with optional crossover to offer all patients potential to receive Iifileucel (NCT05727904)
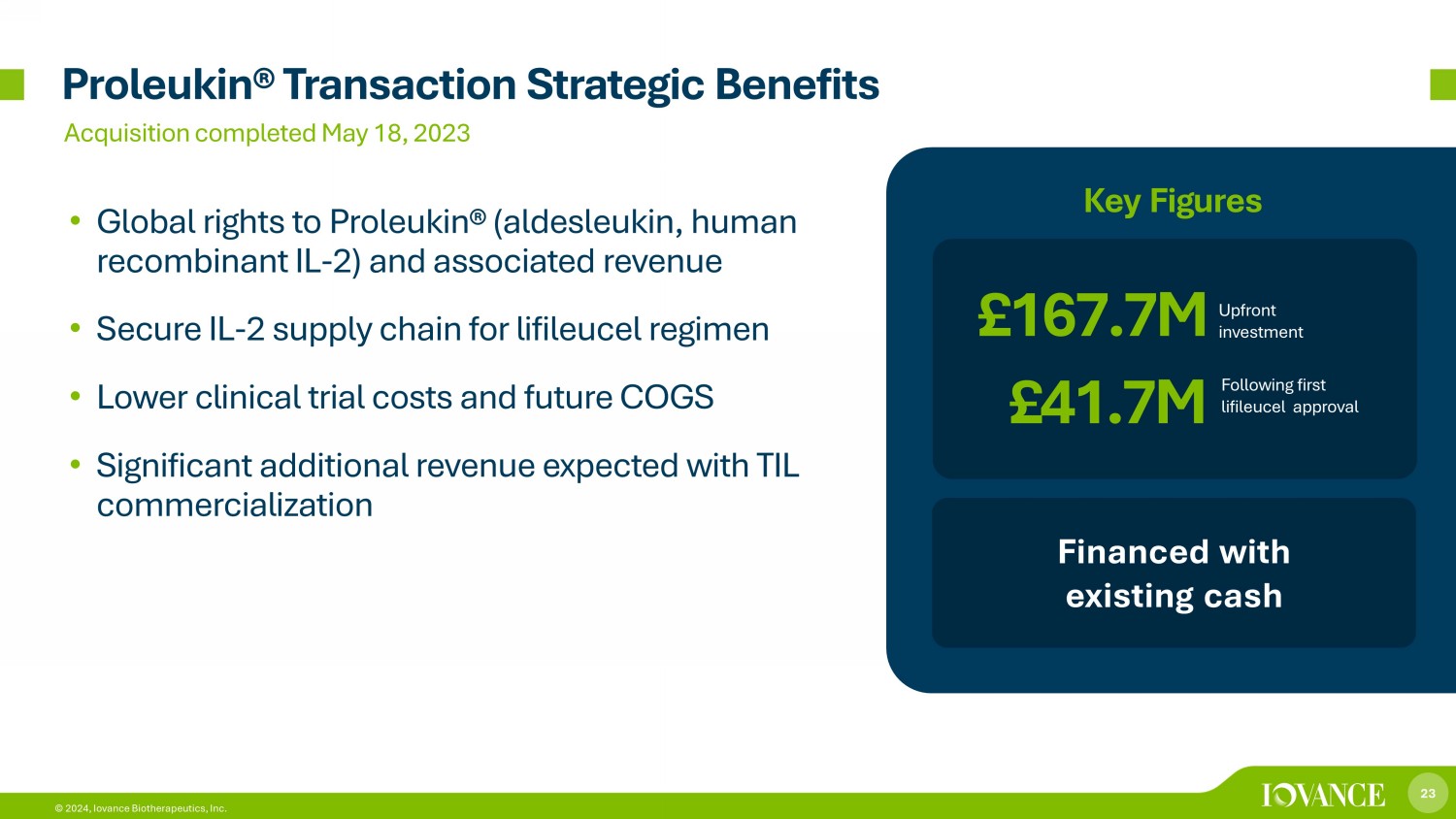
23 © 2024, Iovance Biotherapeutics, Inc. Proleukin® Transaction Strategic Benefits • Global rights to Proleukin® (aldesleukin, human recombinant IL - 2) and associated revenue • Secure IL - 2 supply chain for lifileucel regimen • Lower clinical trial costs and future COGS • Significant additional revenue expected with TIL commercialization £167.7M Upfront investment Financed with existing cash Key Figures £41.7M Following first lifileucel approval Acquisition completed May 18, 2023
24 © 2024, Iovance Biotherapeutics, Inc. 24 Iovance TIL Therapy in Non - Small Cell Lung Cancer

25 © 2024, Iovance Biotherapeutics, Inc. 1. National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program. 2023 Estimates. https://seer.cancer.gov acc essed May 2023 2. American Cancer Society, Lung Cancer. https://www.cancer.org/cancer/types/lung - cancer/about.html accessed July 2023 3. National Cancer Database, NSCLC survival from >1 million patients assessed. Lou Y et al. Survival trends among non - small - cell lu ng cancer patients over a decade: impact of initial therapy at academic centers. Cancer Med. 2018. 4. Clarivate DRG Disease Landscape (2021) Abbreviations: EU5=France, Germany, Italy, Spain and United Kingdom; 1L=first line therapy, 2L=second line therapy, 3L=third lin e therapy, 4L=fourth line therapy; mOS=median overall survival Potential Market for Advanced Non - Small Cell Lung Cancer (NSCLC) Addressing a Substantial Unmet Need in Metastatic NSCLC Iovance TIL clinical program: • 6 cohorts across 3 trials • Multiple treatment regimens • Various populations and stages of disease Annual Deaths in U.S. 2 127K annual deaths in U.S. 1 107K 51.6K 19.0K 116K 46.2K 12.3K 1L 2L 3L US EU5 NSCLC Drug - Treated Population in 2022 Stage IV (US and EU5) 4 Leading cause of U.S. cancer deaths, accounting for ~1 in 5 cancer - related deaths 2 9% 5 - year survival rate 2 and real - world overall survival <6 months 3 in U.S.

26 © 2024, Iovance Biotherapeutics, Inc. IOV - LUN - 202 Trial Design Phase 2 Multicenter Study of LN - 145 † in Patients Post - Anti - PD - 1 NSCLC (NCT04614103)* Endpoints • Primary: ORR by IRC • Secondary: Safety * U.S. FDA placed a clinical hold on the IOV - LUN - 202 trial on December 22, 2023 . Enrollment for new patients is paused. Patients previously treated continue to be monitored and followed. Patients who have already undergone tumor resection will continue to receive the LN - 145 TIL treatment regimen with additional precautions and risk mitigations.. † Gen 2 TIL product † † Cohort 3 patients unable to undergo surgical harvest, TIL grown from core biopsy Abbreviations: Anti - PD - 1, anti - programmed cell death inhibitor; IRC, independent review committee; NSCLC, non - small - cell lung ca ncer; ORR, objective response rate; TPS, tumor proportion score Iovance TIL Therapy LN - 145 in NSCLC IOV - LUN - 202 is designed to enroll patients with advanced NSCLC with a high unmet medical need, but limited prior lines of therapy post anti - PD - 1 treatment Patient Population Unresectable or metastatic NSCLC with progression on or after prior anti - PD - 1 treatment and chemotherapy ~40 sites and expanding in U.S., Canada, Europe Cohort 1: NSCLC Patients with < 1% or unknown TPS LN - 145 Cohort 2: NSCLC Patients with ≥ 1% TPS LN - 145 Cohort 3: Core Biopsy and Gen3 †† LN - 145 Cohort 4: LN - 145, pre - PD tumor harvest Retreatment Cohort Exploratory Cohorts Registrational Cohorts
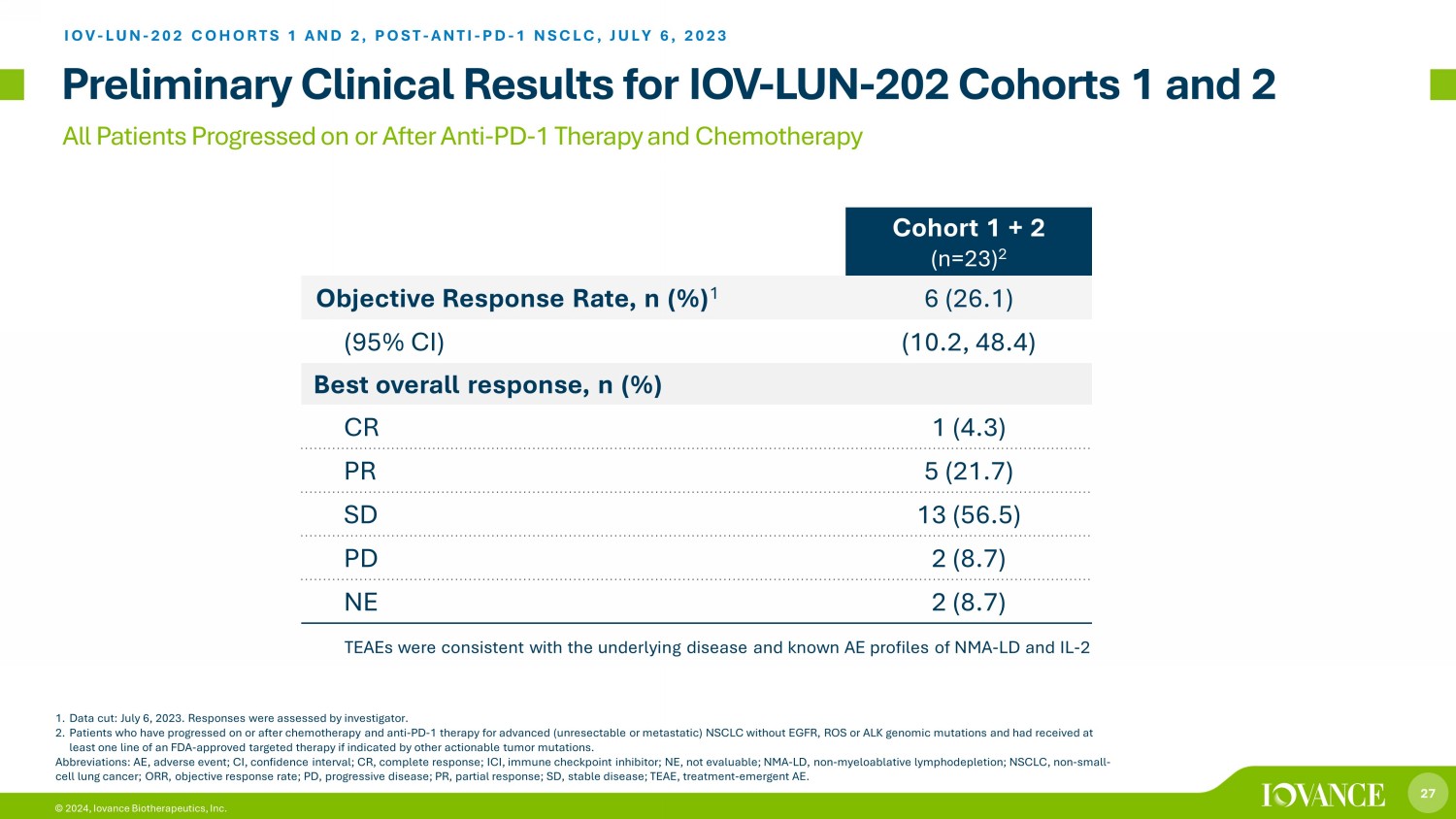
27 © 2024, Iovance Biotherapeutics, Inc. All Patients Progressed on or After Anti - PD - 1 Therapy and Chemotherapy Preliminary Clinical Results for IOV - LUN - 202 Cohorts 1 and 2 1. Data cut: July 6, 2023. Responses were assessed by investigator. 2. Patients who have progressed on or after chemotherapy and anti - PD - 1 therapy for advanced (unresectable or metastatic) NSCLC with out EGFR, ROS or ALK genomic mutations and had received at least one line of an FDA - approved targeted therapy if indicated by other actionable tumor mutations. Abbreviations: AE, adverse event; CI, confidence interval; CR, complete response; ICI, immune checkpoint inhibitor; NE, not e val uable; NMA - LD, non - myeloablative lymphodepletion; NSCLC, non - small - cell lung cancer; ORR, objective response rate; PD, progressive disease; PR, partial response; SD, stable disease; TEAE, trea tme nt - emergent AE. Iovance TIL Therapy LN - 145 in NSCLC Cohort 1 + 2 (n=23) 2 Objective Response Rate, n (%) 1 6 (26.1) (95% CI) (10.2, 48.4) Best overall response, n (%) CR 1 (4.3) PR 5 (21.7) SD 13 (56.5) PD 2 (8.7) NE 2 (8.7) IOV - LUN - 202 COHORTS 1 AND 2, POST - ANTI - PD - 1 NSCLC, JULY 6, 2023 TEAEs were consistent with the underlying disease and known AE profiles of NMA - LD and IL - 2
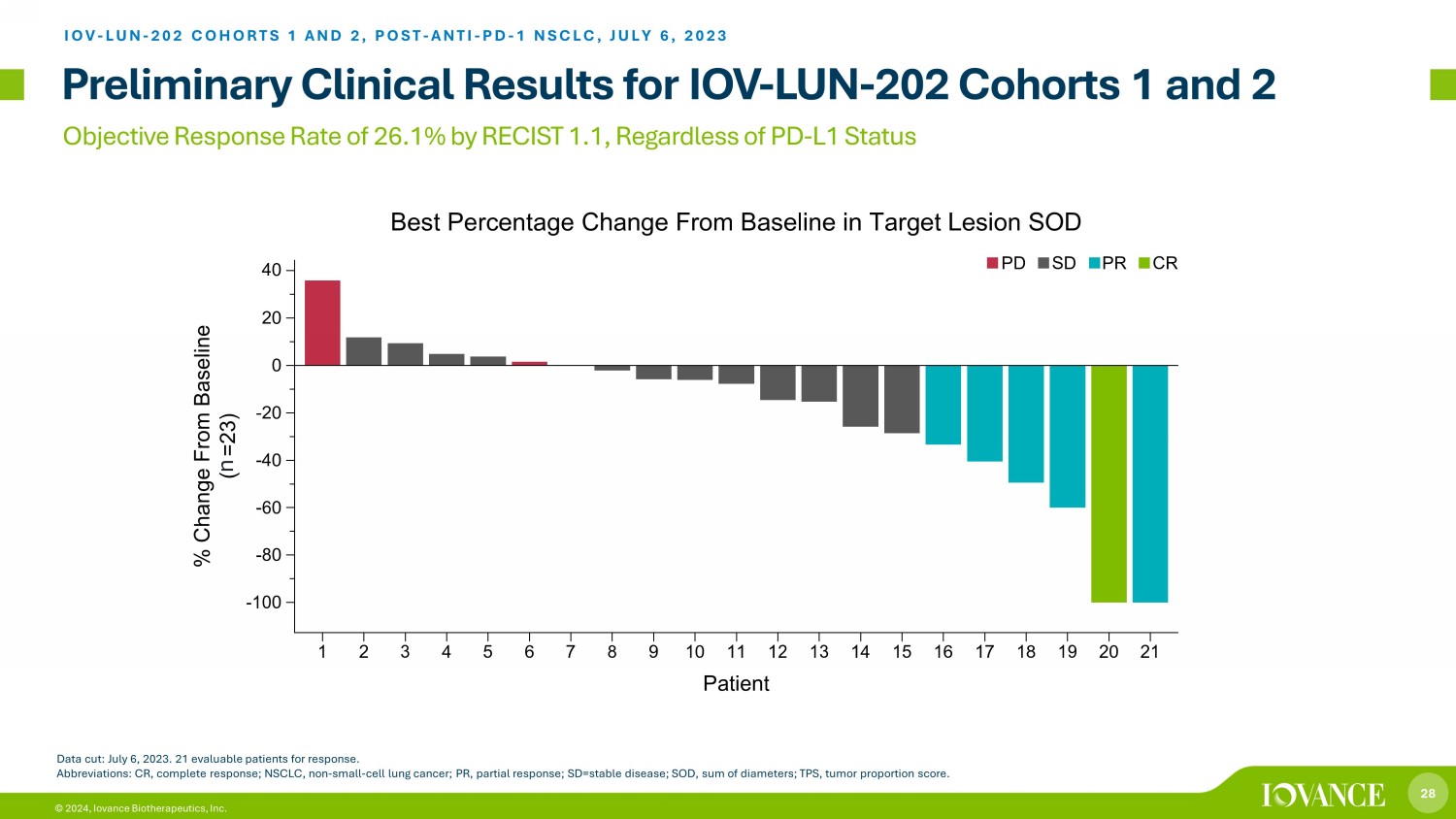
28 © 2024, Iovance Biotherapeutics, Inc. Objective Response Rate of 26.1% by RECIST 1.1, Regardless of PD - L1 Status Preliminary Clinical Results for IOV - LUN - 202 Cohorts 1 and 2 IOV - LUN - 202 COHORTS 1 AND 2, POST - ANTI - PD - 1 NSCLC, JULY 6, 2023 Data cut: July 6, 2023. 21 evaluable patients for response. Abbreviations: CR, complete response; NSCLC, non - small - cell lung cancer; PR, partial response; SD=stable disease; SOD, sum of di ameters; TPS, tumor proportion score. n
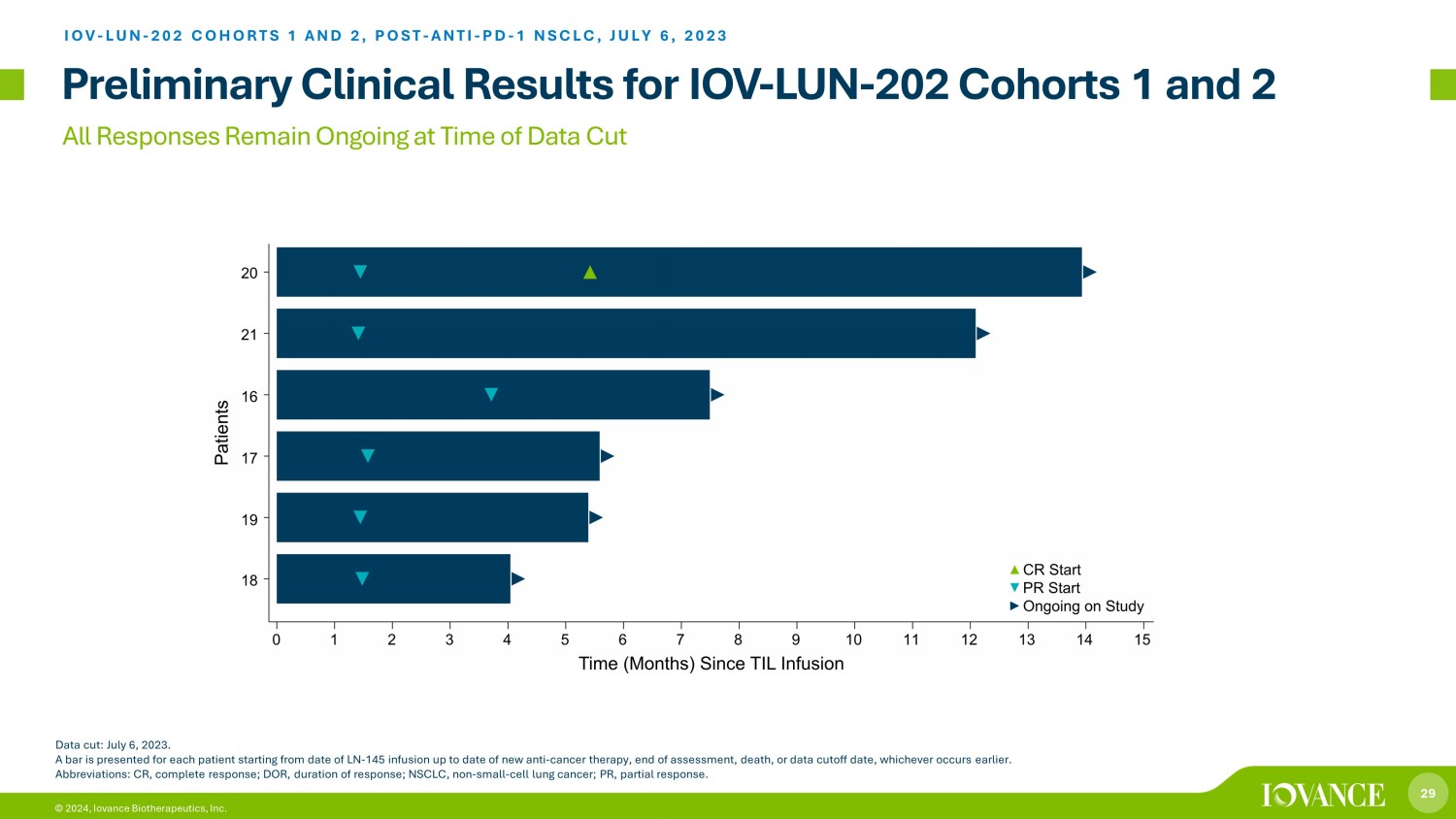
29 © 2024, Iovance Biotherapeutics, Inc. All Responses Remain Ongoing at Time of Data Cut Data cut: July 6, 2023. A bar is presented for each patient starting from date of LN - 145 infusion up to date of new anti - cancer therapy, end of assessme nt, death, or data cutoff date, whichever occurs earlier. Abbreviations: CR, complete response; DOR, duration of response; NSCLC, non - small - cell lung cancer; PR, partial response. IOV - LUN - 202 COHORTS 1 AND 2, POST - ANTI - PD - 1 NSCLC, JULY 6, 2023 Preliminary Clinical Results for IOV - LUN - 202 Cohorts 1 and 2
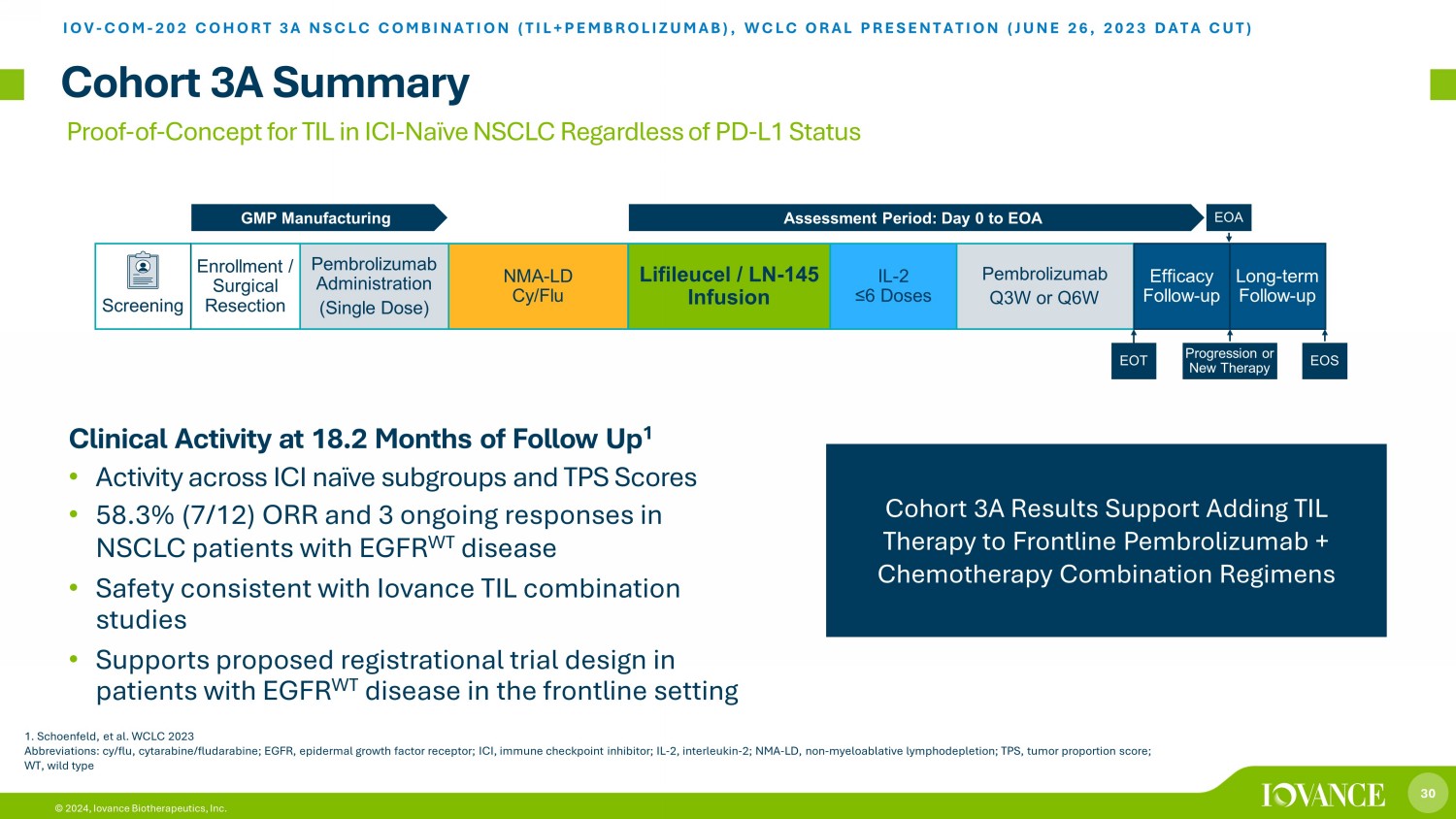
30 © 2024, Iovance Biotherapeutics, Inc. Proof - of - Concept for TIL in ICI - Naïve NSCLC Regardless of PD - L1 Status Cohort 3A Summary IOV - COM - 202 COHORT 3A NSCLC COMBINATION (TIL+PEMBROLIZUMAB ), WCLC ORAL PRESENTATION (JUNE 26, 2023 DATA CUT) Cohort 3A Results Support Adding TIL Therapy to Frontline Pembrolizumab + Chemotherapy Combination Regimens Clinical Activity at 18.2 Months of Follow Up 1 • Activity across ICI naïve subgroups and TPS Scores • 58.3% (7/12) ORR and 3 ongoing responses in NSCLC patients with EGFR WT disease • Safety consistent with Iovance TIL combination studies • Supports proposed registrational trial design in patients with EGFR WT disease in the frontline setting Screening Pembrolizumab Administration (Single Dose) NMA - LD Cy/Flu Lifileucel / LN - 145 Infusion IL - 2 ≤6 Doses Pembrolizumab Q3W or Q6W Efficacy Follow - up Enrollment / Surgical Resection Assessment Period: Day 0 to EOA GMP Manufacturing EOA Progression or New Therapy EOS EOT Long - term Follow - up 1. Schoenfeld, et al. WCLC 2023 Abbreviations: cy/flu, cytarabine/fludarabine; EGFR, epidermal growth factor receptor; ICI, immune checkpoint inhibitor; IL - 2, interleukin - 2; NMA - LD, non - myeloablative lymphodepletion; TPS, tumor proportion score; WT, wild type
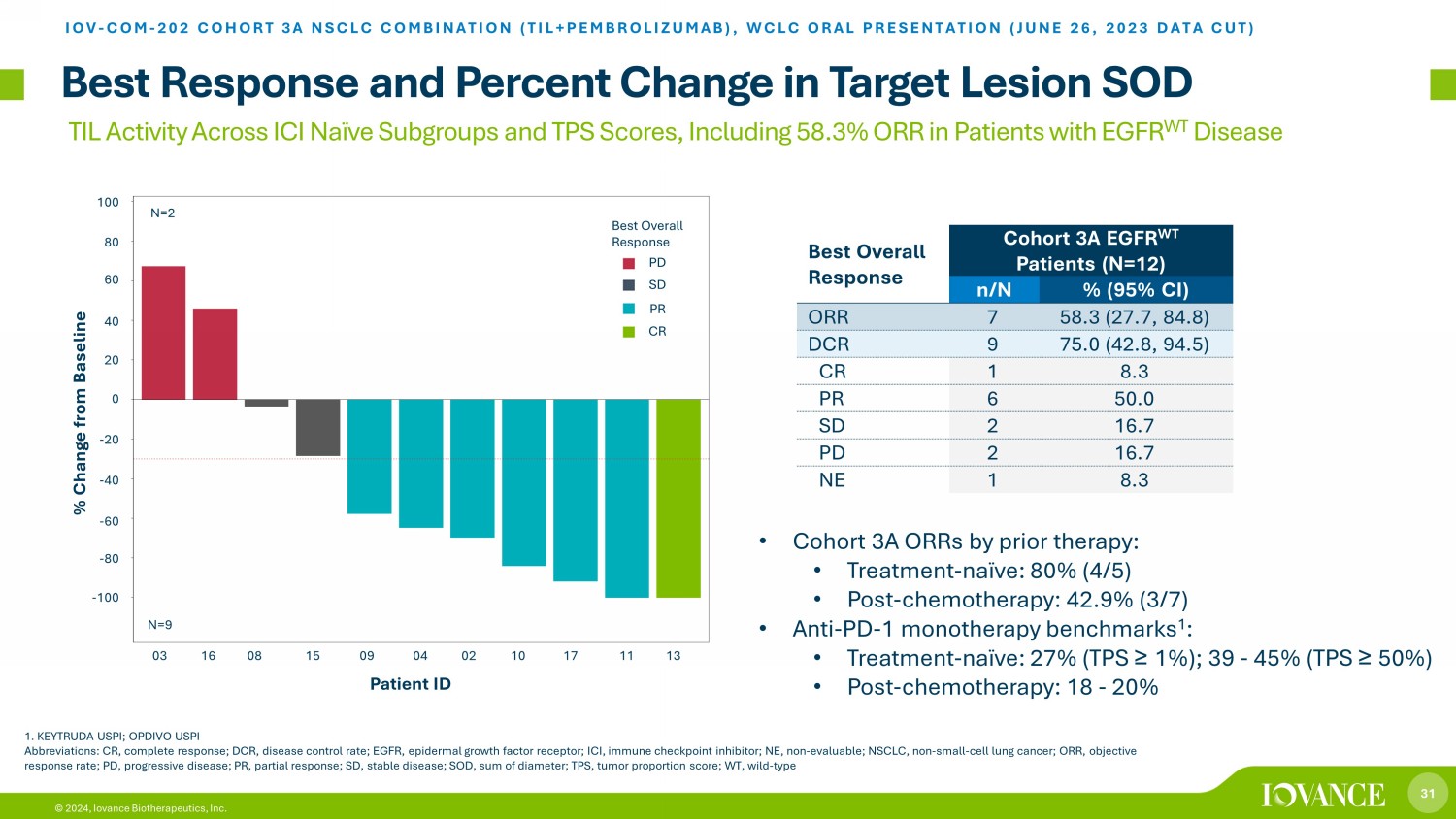
31 © 2024, Iovance Biotherapeutics, Inc. TIL Activity Across ICI Naïve Subgroups and TPS Scores, Including 58.3% ORR in Patients with EGFR WT Disease Best Response and Percent Change in Target Lesion SOD IOV - COM - 202 COHORT 3A NSCLC COMBINATION (TIL+PEMBROLIZUMAB ), WCLC ORAL PRESENTATION (JUNE 26, 2023 DATA CUT) 1. KEYTRUDA USPI; OPDIVO USPI Abbreviations: CR, complete response; DCR, disease control rate; EGFR, epidermal growth factor receptor; ICI, immune checkpoi nt inhibitor; NE, non - evaluable; NSCLC, non - small - cell lung cancer; ORR, objective response rate; PD, progressive disease; PR, partial response; SD, stable disease; SOD, sum of diameter; TPS, tumor proportion sc ore; WT, wild - type Best Overall Response Cohort 3A EGFR WT Patients (N=12) n/N % (95% CI) ORR 7 58.3 (27.7, 84.8) DCR 9 75.0 (42.8, 94.5) CR 1 8.3 PR 6 50.0 SD 2 16.7 PD 2 16.7 NE 1 8.3 • Cohort 3A ORRs by prior therapy: • Treatment - naïve: 80% (4/5) • Post - chemotherapy: 42.9% (3/7) • Anti - PD - 1 monotherapy benchmarks 1 : • Treatment - naïve: 27% (TPS ≥ 1%); 39 - 45% (TPS ≥ 50%) • Post - chemotherapy: 18 - 20% 60 40 20 0 - 20 - 40 - 60 - 80 3A-03 3A-16 3A-08 3A-15 3A-09 3A-04 3A-02 3A-10 3A-17 3A-11 3A-13 -100 -80 -60 -40 -20 0 20 40 60 80 100 % C h a n g e f r o m B a s e l i n e N=2 N=9 CRPRSDPD Best Overall Response Patient ID 03 16 08 15 09 04 02 10 17 11 13 - 100 - 80 - 60 - 40 - 20 0 20 40 60 80 100 % Change from Baseline N=9 N=2 Best Overall Response PD SD PR CR

32 © 2024, Iovance Biotherapeutics, Inc. Time on Study for Confirmed EGFR WT Responders (n=7) IOV - COM - 202 COHORT 3A NSCLC COMBINATION (TIL+PEMBROLIZUMAB ), WCLC ORAL PRESENTATION (JUNE 26, 2023 DATA CUT) Durable Responses Include 3 Ongoing Responders with EGFR WT Disease at a Median Study Follow up of 18.2 Months A bar for each patient starts from date of LN - 145 infusion up to date of new anti - cancer therapy, end of assessment, death, or d ata cutoff date, whichever occurs earlier. a. As adjudicated between site - reported and central - laboratory data; b. Patient received prior neoadjuvant chemoradiotherapy; Abbreviations: BOR, best overall response; CR, complete response; NSCLC, non - small - cell lung cancer; NSQ, nonsquamous; ORR, obje ctive response rate; PD - L1, programmed death ligand 1; PR, partial response; Pt, patient; SOD, sum of diameters; SQ, squamous; TPS, tumor proportion score; WT, wild - type 3A-10 3A-09 3A-17 3A-04 3A-02 3A-13 3A-11 S u b j e c t s 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Time (months) since TIL Infusion Pembro Infusion Progression Ongoing on Study PR Start CR Start Pt ID Prior ICI Prior Chemo PD - L1 TPS a (%) SQ or NSQ BOR 11 No Yes <1 NSQ PR 13 No Yes <1 NSQ CR 2 No No b <1 NSQ PR 4 No No ≥ 50 NSQ PR 17 No No ≥ 50 SQ PR 9 No Yes <1 NSQ PR 10 No No ≥ 50 NSQ PR 0 1 5 7 8 2 3 4 6 9 10 16 11 12 13 14 15 22 17 18 19 20 21 23 Time (Months) Since TIL Infusion

33 © 2024, Iovance Biotherapeutics, Inc. Deepening of Responses Over Time are Characteristic of One - Time Immunotherapy Change in Target Lesion SOD in EGFR WT Patients (n=11) IOV - COM - 202 COHORT 3A NSCLC COMBINATION (TIL+PEMBROLIZUMAB ), WCLC ORAL PRESENTATION (JUNE 26, 2023 DATA CUT) Abbreviations: CR, complete response; EGFR, epidermal growth factor receptor; NSCLC, non - small - cell lung cancer; PR, partial res ponse; SD, stable disease; PD, progressive disease; WT, wild - type Best Overall Response PD SD PR CR Visit 60 40 - 100 - 80 - 60 - 40 - 20 0 20 40 60 80 Baseline % Change from Baseline Day 42 Day 84 Day 126 Month 6 Month 9 Month 12 Month 15 Month 18 Pt 3 (PD) Pt 8 (SD) Pt 15 (SD) Pt 9 (PR) Pt 10 (PR) Pt 17 (PR*) Pt 13 (CR*) Pt 11 (PR*) Pt 4 (PR) *Ongoing Response Pt 16 (PD) Pt 2 (PR) 3A-16 (PD) 3A-03 (PD) 3A-15 (SD) 3A-08 (SD) 3A-04 (PR) 3A-11 (PR) 3A-17 (PR) 3A-02 (PR) 3A-10 (PR) 3A-09 (PR) 3A-13 (CR) Baseline Day 42 Day 84 Day 126 Month 6 Month 9 Month 12 Month 15 Month 18 Visit -100 -80 -60 -40 -20 0 20 40 60 80 P e r c e n t C h a n g e CRPRSDPD Best Response
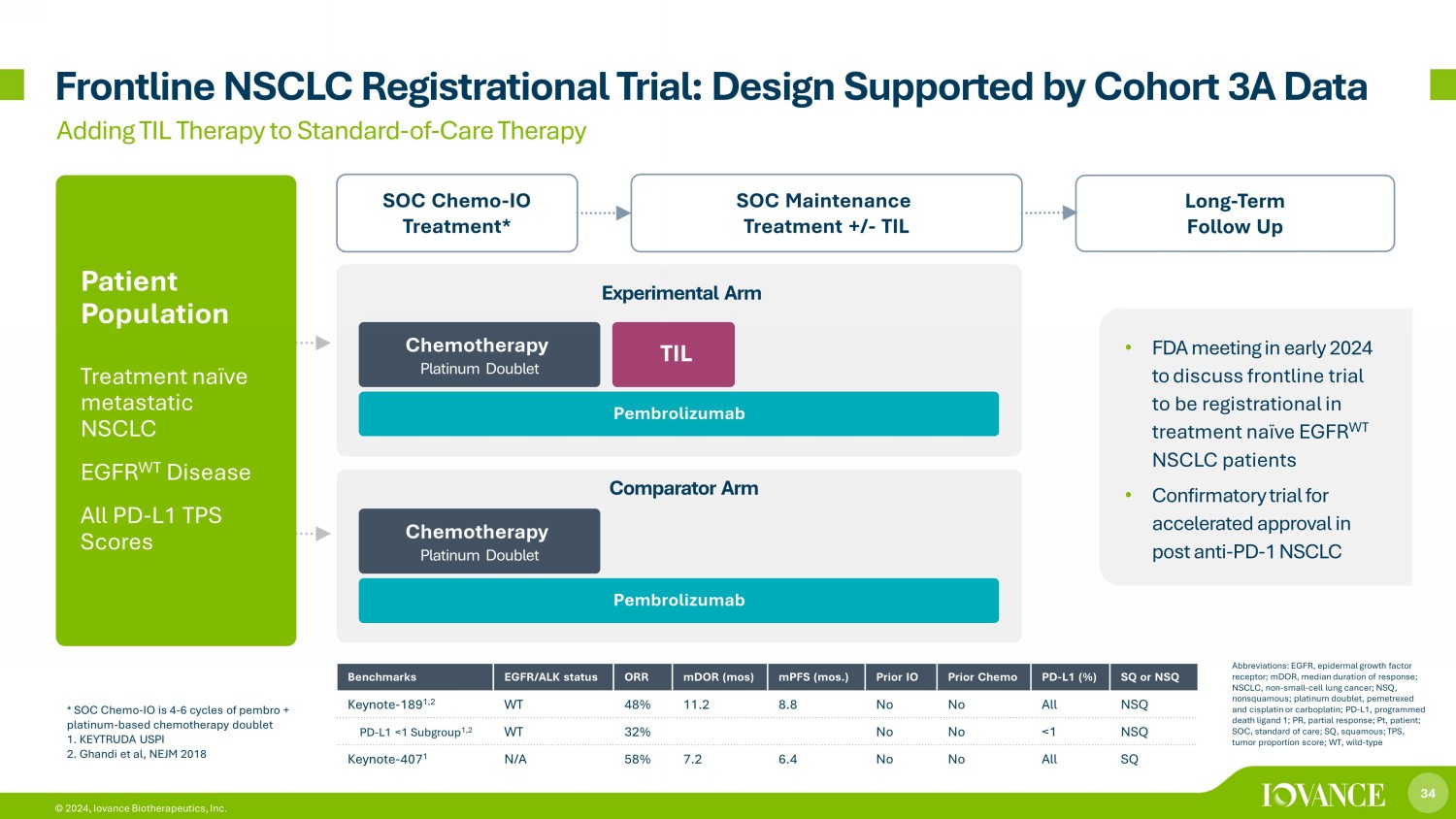
34 © 2024, Iovance Biotherapeutics, Inc. Frontline NSCLC Registrational Trial: Design Supported by Cohort 3A Data Long - Term Follow Up SOC Maintenance Treatment +/ - TIL SOC Chemo - IO Treatment* Adding TIL Therapy to Standard - of - Care Therapy TIL Patient Population Treatment naïve metastatic NSCLC EGFR WT Disease All PD - L1 TPS Scores Chemotherapy Platinum Doublet * SOC Chemo - IO is 4 - 6 cycles of pembro + platinum - based chemotherapy doublet 1. KEYTRUDA USPI 2. Ghandi et al, NEJM 2018 Benchmarks EGFR/ALK status ORR mDOR (mos) mPFS (mos.) Prior IO Prior Chemo PD - L1 (%) SQ or NSQ Keynote - 189 1,2 WT 48% 11.2 8.8 No No All NSQ PD - L1 <1 Subgroup 1,2 WT 32% No No <1 NSQ Keynote - 407 1 N/A 58% 7.2 6.4 No No All SQ Experimental Arm Pembrolizumab Comparator Arm Abbreviations: EGFR, epidermal growth factor receptor; mDOR, median duration of response; NSCLC, non - small - cell lung cancer; NSQ, nonsquamous; platinum doublet, pemetrexed and cisplatin or carboplatin; PD - L1, programmed death ligand 1; PR, partial response; Pt, patient; SOC, standard of care; SQ, squamous; TPS, tumor proportion score; WT, wild - type Chemotherapy Platinum Doublet Pembrolizumab • FDA meeting in early 2024 to discuss frontline trial to be registrational in treatment naïve EGFR WT NSCLC patients • Confirmatory trial for accelerated approval in post anti - PD - 1 NSCLC
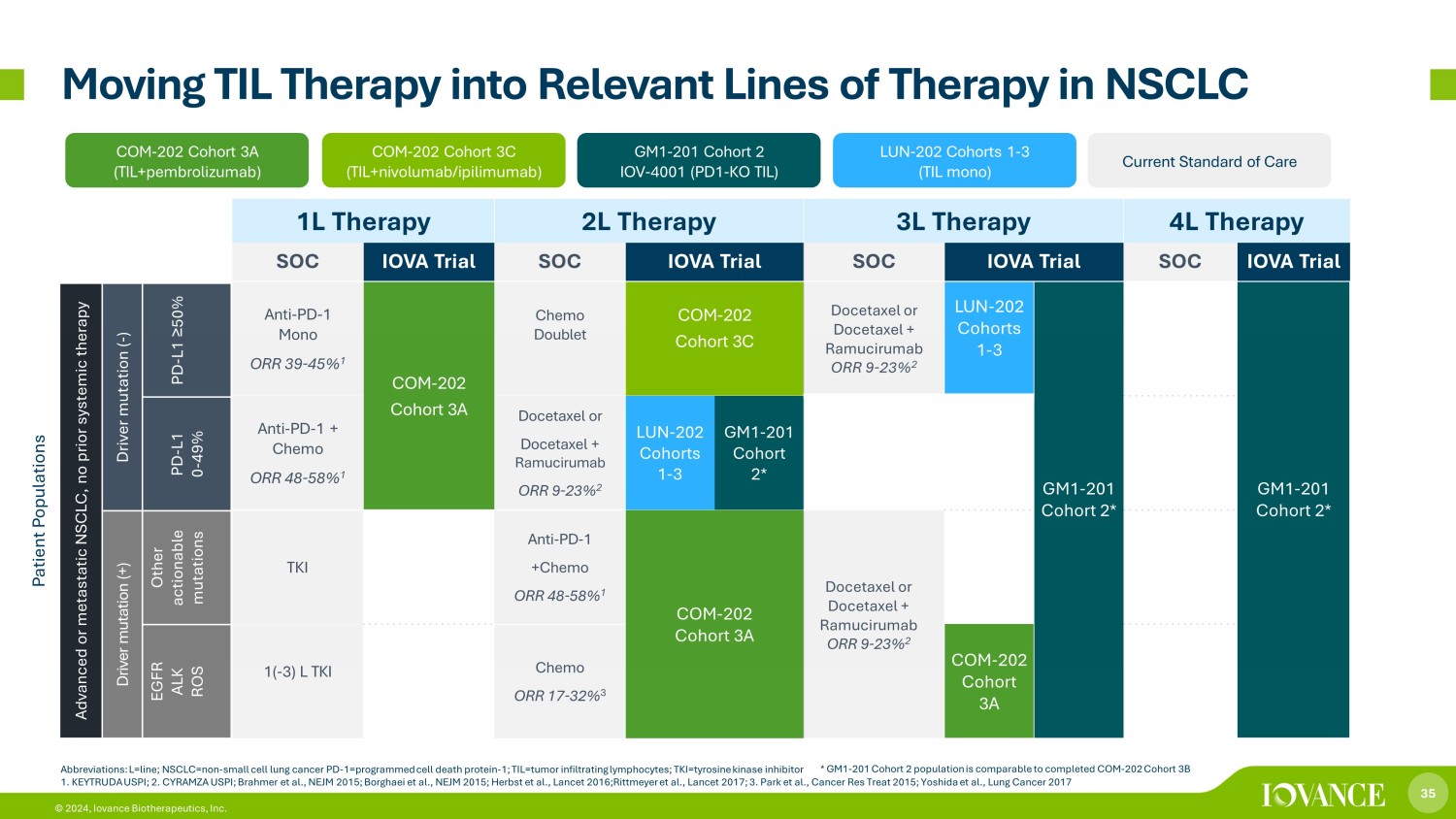
35 © 2024, Iovance Biotherapeutics, Inc. 1L Therapy 2L Therapy 3L Therapy 4L Therapy SOC IOVA Trial SOC IOVA Trial SOC IOVA Trial SOC IOVA Trial Anti - PD - 1 Mono ORR 39 - 45% 1 COM - 202 Cohort 3A Chemo Doublet COM - 202 Cohort 3C Docetaxel or Docetaxel + Ramucirumab ORR 9 - 23% 2 LUN - 202 Cohorts 1 - 3 GM1 - 201 Cohort 2* GM1 - 201 Cohort 2* Anti - PD - 1 + Chemo ORR 48 - 58% 1 Docetaxel or Docetaxel + Ramucirumab ORR 9 - 23% 2 LUN - 202 Cohorts 1 - 3 GM1 - 201 Cohort 2* TKI Anti - PD - 1 +Chemo ORR 48 - 58% 1 COM - 202 Cohort 3A Docetaxel or Docetaxel + Ramucirumab ORR 9 - 23% 2 1( - 3) L TKI Chemo ORR 17 - 32% 3 COM - 202 Cohort 3A * GM1 - 201 Cohort 2 population is comparable to completed COM - 202 Cohort 3B Moving TIL Therapy into Relevant Lines of Therapy in NSCLC COM - 202 Cohort 3A (TIL+pembrolizumab) LUN - 202 Cohorts 1 - 3 (TIL mono) COM - 202 Cohort 3C (TIL+ nivolumab / i pilimumab) GM1 - 201 Cohort 2 IOV - 4001 (PD1 - KO TIL) Current Standard of Care Patient Populations Advanced or metastatic NSCLC, no prior systemic therapy Driver mutation ( - ) PD - L1 ≥ 50% PD - L1 0 - 49% Driver mutation (+) Other actionable mutations EGFR ALK ROS Abbreviations: L=line; NSCLC=non - small cell lung cancer PD - 1=programmed cell death protein - 1; TIL=tumor infiltrating lymphocytes ; TKI=tyrosine kinase inhibitor 1. KEYTRUDA USPI; 2. CYRAMZA U S PI; Brahmer et al., NEJM 2015; Borghaei et al., NEJM 2015; Herbst et al., Lancet 2016;Rittmeyer et al., Lancet 2017; 3. Park et al., Cancer Res Treat 2015; Yoshida et al., Lung Cancer 2017

36 © 2024, Iovance Biotherapeutics, Inc. 36 Launch Preparation

37 © 2024, Iovance Biotherapeutics, Inc. i CTC Designed for High - Volume TIL Manufacturing and Flexibility • Core suites: TIL commercial manufacturing • Flexible suites: clinical supply, pipeline expansion and advanced manufacturing • Integrated quality control, supply chain and IT systems • 100+ employees with additional staffing into launch and beyond • iCTC supplemented with external CDMO manufacturing capacity 37 © 2024, Iovance Biotherapeutics, Inc.

38 © 2024, Iovance Biotherapeutics, Inc. Targeting Potential Authorized Treatment Centers (ATCs) Potential ATC Iovance Clinical Trial Site 1 1. ClinicalTrials.gov Abbreviations: ATC=Authorized Treatment Centers; NCCN=National Comprehensive Cancer Network; KOL=Key Opinion Leaders; BMT=Bone Marrow Transplant Targeting Considerations • Patient volume • NCCN status, KOLs • Existing cell therapy / BMT • Inpatient capacity • Iovance clinical trial (s) Drive Demand • Top account prioritization • Community referrals ~30 ATCs Completed Pre - Approval Onboarding; ~50 ATCs Expected 90 Days Post - PDUFA

39 © 2024, Iovance Biotherapeutics, Inc. 55% Commercial Medicare IPPS Exempt 4% 17% Medicare Advantage 8% Medicare FFS 7% Medicaid 9% Other Enabling Market Access Metastatic Melanoma Payer Mix 1 All Treatment Settings and Lines of Therapy 1. Metastatic Melanoma Insurance Claims Analysis, TIL - eligible patients treated in the ATC setting(1/1/2018 – 6/30/2021). Medicai d is 6% Medicaid Advantage and 1% Medicaid Fee - For - Service; For the 12% Medicare FFS lives, 11 PPS - exempt hospitals are reimbursed by Medicare FFS on a cost - basis (~4%), with the remaining Medicare FFS lives (~8%) reimbursed under DRG - 018 payment methodology, NTAP/Outlier payments may add to the total Medicare reimbursement. Other segment includes cash, self - insured, VA, and other unidentifiable claims. Abbreviations: FFS=Fee - For - Service; ICD - 10 PCS=International Classification of Diseases, 10 th Revision, Procedure Coding System; NTAP = New Technology Add - on Payment Payers appreciate the high unmet need, lack of treatment options, and lifileucel clinical value Anticipated Access • Engagement with payers responsible for ~90% of covered lives • Strong hospital reimbursement expected ̶ Inpatient payment methodologies are established ̶ Key payers expected to reimburse majority of provider costs • Expect similar coverage to CAR - Ts
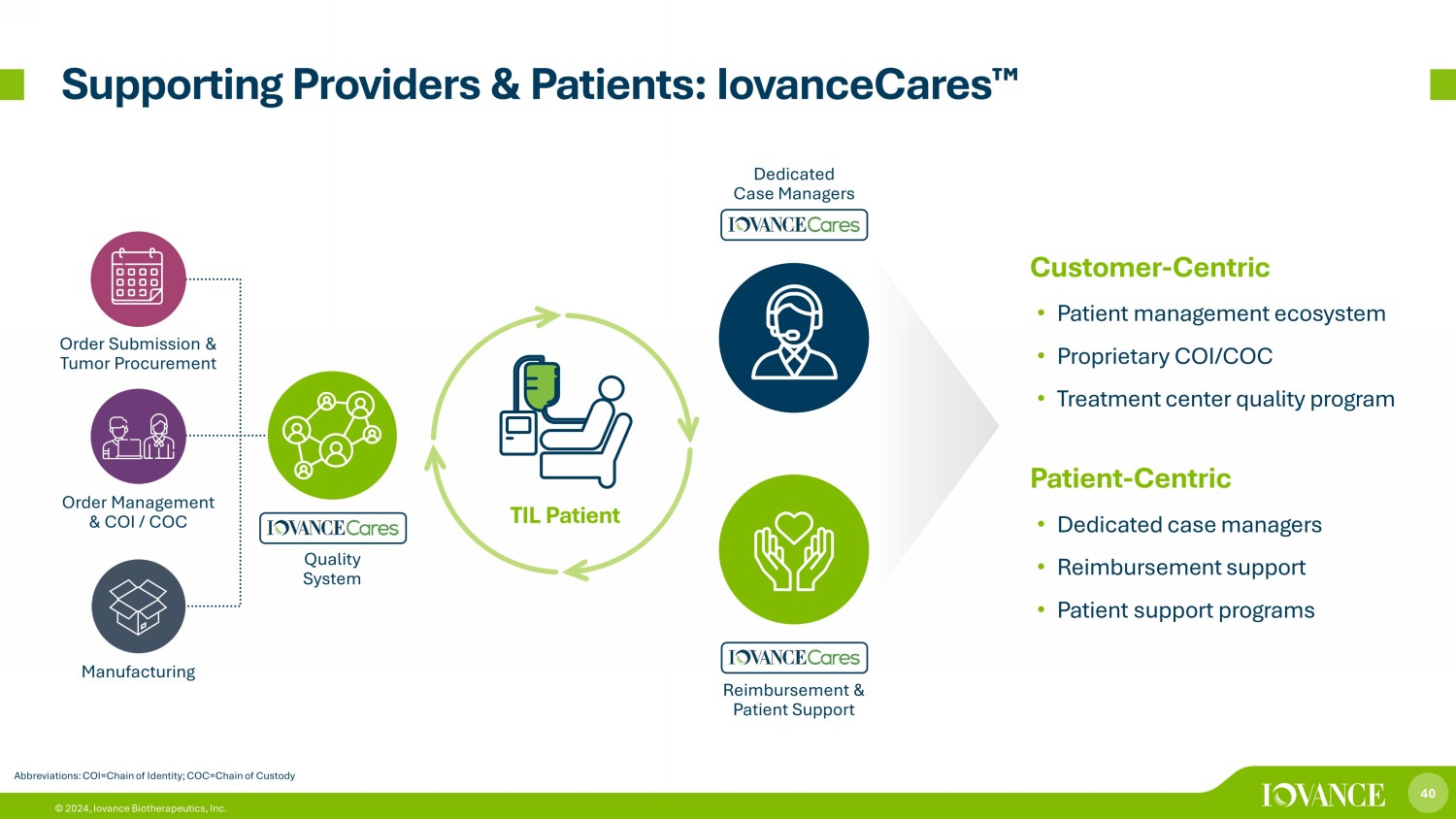
40 © 2024, Iovance Biotherapeutics, Inc. Supporting Providers & Patients: IovanceCares ¯ Abbreviations: COI=Chain of Identity; COC=Chain of Custody Customer - Centric • Patient management ecosystem • Proprietary COI/COC • Treatment center quality program Patient - Centric • Dedicated case managers • Reimbursement support • Patient support programs Quality System Dedicated Case Managers Reimbursement & Patient Support Order Submission & Tumor Procurement Order Management & COI / COC Manufacturing TIL Patient
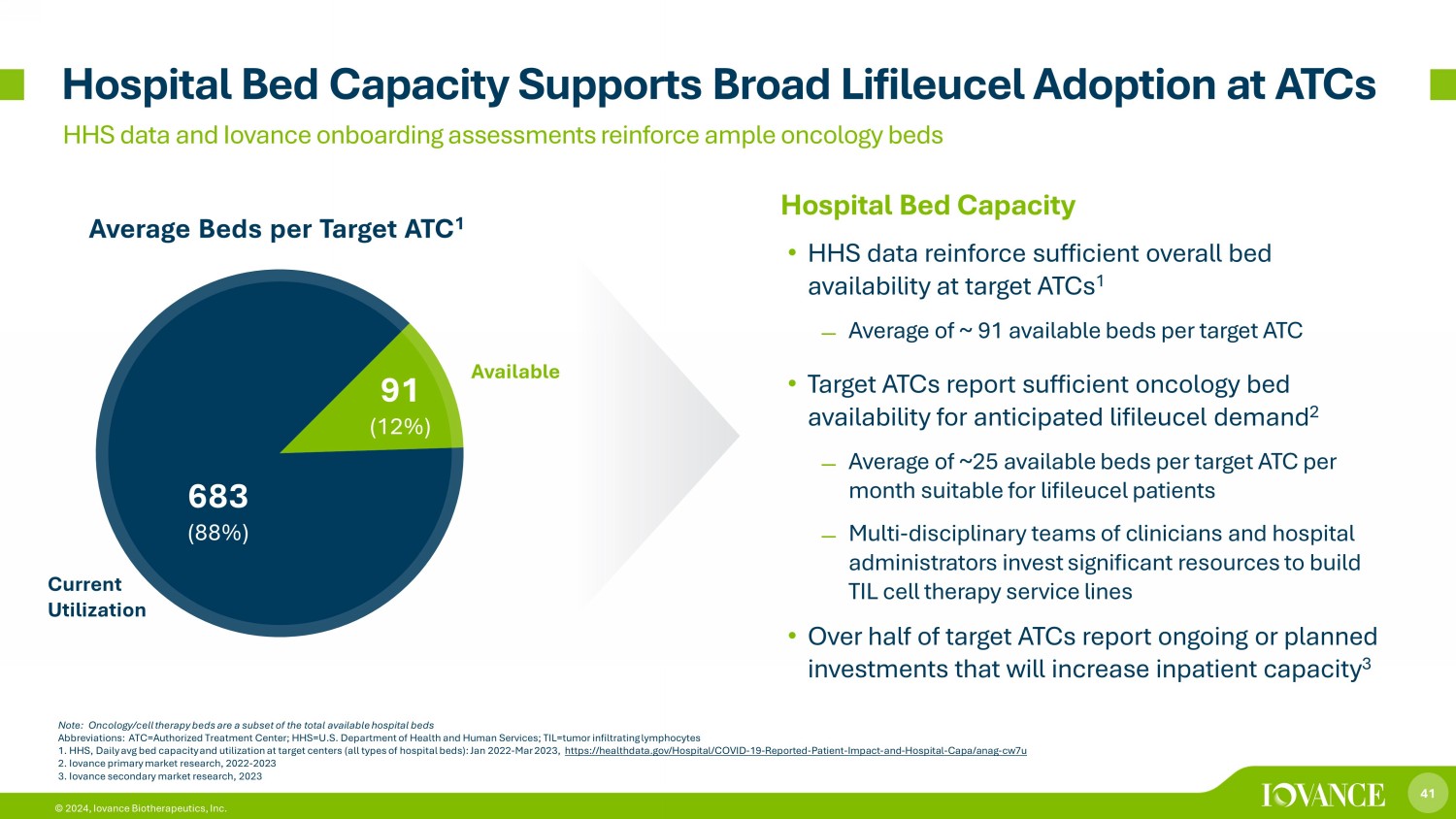
41 © 2024, Iovance Biotherapeutics, Inc. Hospital Bed Capacity • HHS data reinforce sufficient overall bed availability at target ATCs 1 ̶ Average of ~ 91 available beds per target ATC • Target ATCs report sufficient oncology bed availability for anticipated lifileucel demand 2 ̶ Average of ~25 available beds per target ATC per month suitable for lifileucel patients ̶ Multi - disciplinary teams of clinicians and hospital administrators invest significant resources to build TIL cell therapy service lines • Over half of target ATCs report ongoing or planned investments that will increase inpatient capacity 3 Average Beds per Target ATC 1 Hospital Bed Capacity Supports Broad Lifileucel Adoption at ATCs HHS data and Iovance onboarding assessments reinforce ample oncology beds Note: Oncology/cell therapy beds are a subset of the total available hospital beds Abbreviations: ATC=Authorized Treatment Center; HHS=U.S. Department of Health and Human Services; TIL=tumor infiltrating lympho cytes 1. HHS, Daily avg bed capacity and utilization at target centers (all types of hospital beds): Jan 2022 - Mar 2023, https://healthdata.gov/Hospital/COVID - 19 - Reported - Patient - Impact - and - Hospital - Capa/anag - cw7u 2. Iovance primary market research, 2022 - 2023 3. Iovance secondary market research, 2023 683 (88%) 91 (12%) Current Utilization Available

42 © 2024, Iovance Biotherapeutics, Inc. 42 Other TIL Therapy Clinical Program Highlights
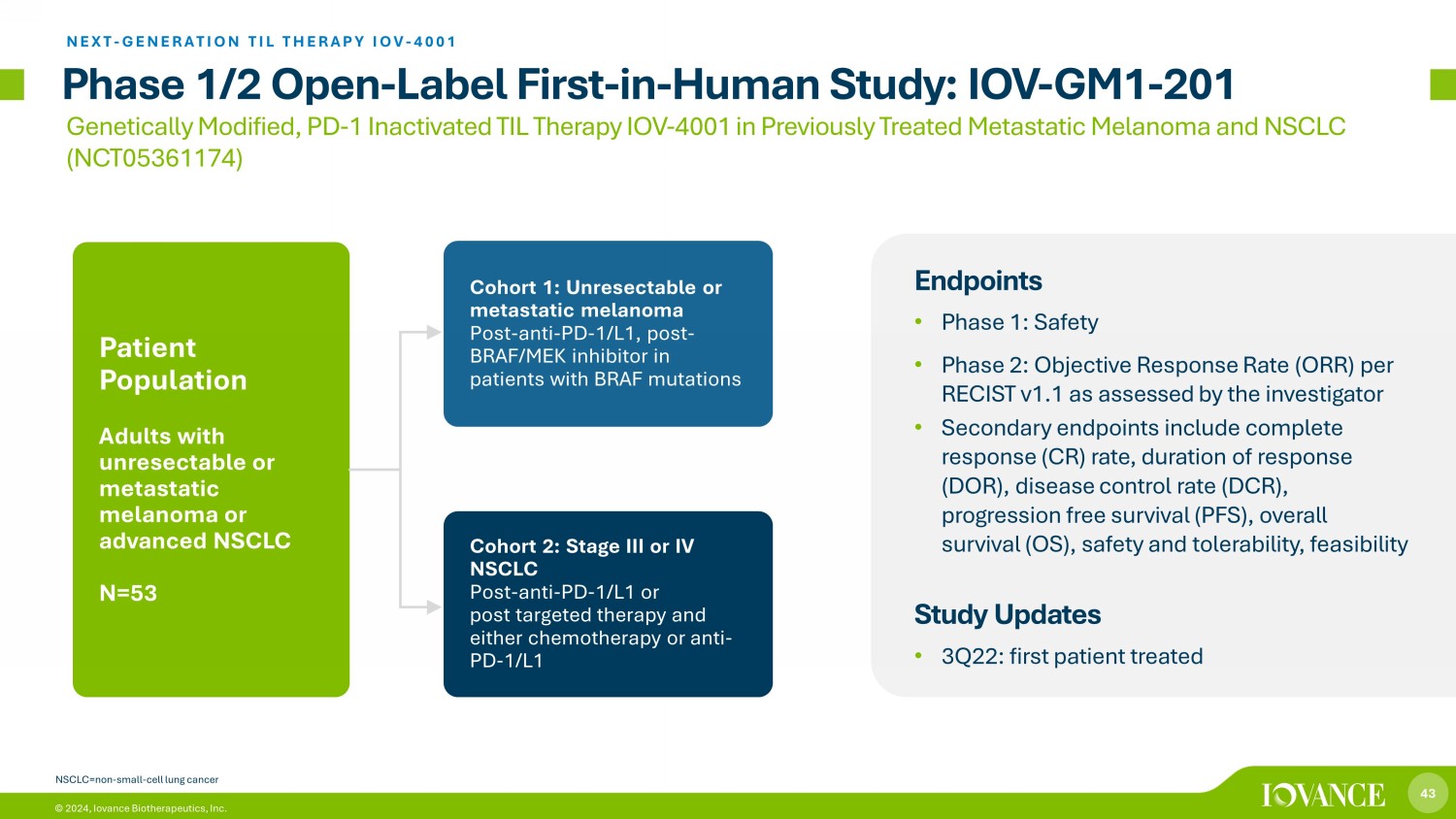
43 © 2024, Iovance Biotherapeutics, Inc. Phase 1/2 Open - Label First - in - Human Study: IOV - GM1 - 201 Endpoints • Phase 1: Safety • Phase 2: Objective Response Rate (ORR) per RECIST v1.1 as assessed by the investigator • Secondary endpoints include complete response (CR) rate, duration of response (DOR), disease control rate (DCR), progression free survival (PFS), overall survival (OS), safety and tolerability, feasibility Study Updates • 3Q22: first patient treated Cohort 1: Unresectable or metastatic melanoma Post - anti - PD - 1/L1, post - BRAF/MEK inhibitor in patients with BRAF mutations Cohort 2: Stage III or IV NSCLC Post - anti - PD - 1/L1 or post targeted therapy and either chemotherapy or anti - PD - 1/L1 Patient Population Adults with unresectable or metastatic melanoma or advanced NSCLC N=53 Genetically Modified, PD - 1 Inactivated TIL Therapy IOV - 4001 in Previously Treated Metastatic Melanoma and NSCLC (NCT05361174) NEXT - GENERATION TIL THERAPY IOV - 4001 NSCLC=non - small - cell lung cancer
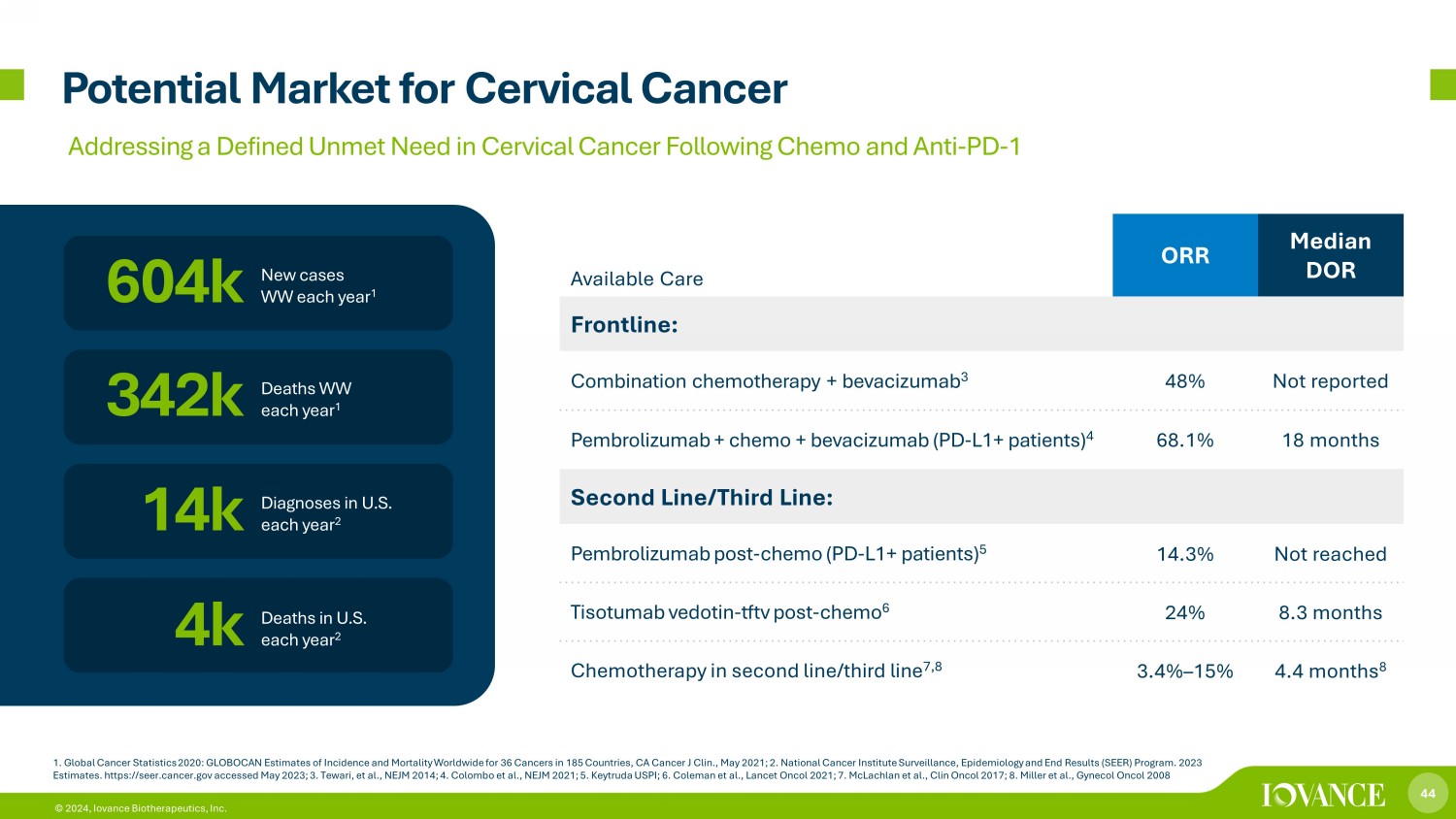
44 © 2024, Iovance Biotherapeutics, Inc. Potential Market for Cervical Cancer 1. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries, CA Ca ncer J Clin., May 2021; 2. National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program. 2023 Estimates. https://seer.cancer.gov accessed May 2023; 3. Tewari, et al., NEJM 2014; 4. Colombo et al., NEJM 2021; 5. Keytruda US PI; 6. Coleman et al., Lancet Oncol 2021; 7. McLachlan et al., Clin Oncol 2017; 8. Miller et al., Gynecol Oncol 2008 New cases WW each year 1 604k 14k Diagnoses in U.S. each year 2 342k 4k Deaths WW each year 1 Deaths in U.S. each year 2 Available Care ORR Median DOR Frontline: Combination chemotherapy + bevacizumab 3 48% Not reported Pembrolizumab + chemo + bevacizumab (PD - L1+ patients) 4 68.1% 18 months Second Line/Third Line: Pembrolizumab post - chemo (PD - L1+ patients) 5 14.3% Not reached Tisotumab vedotin - tftv post - chemo 6 24% 8.3 months Chemotherapy in second line/third line 7,8 3.4% – 15% 4.4 months 8 Addressing a Defined Unmet Need in Cervical Cancer Following Chemo and Anti - PD - 1
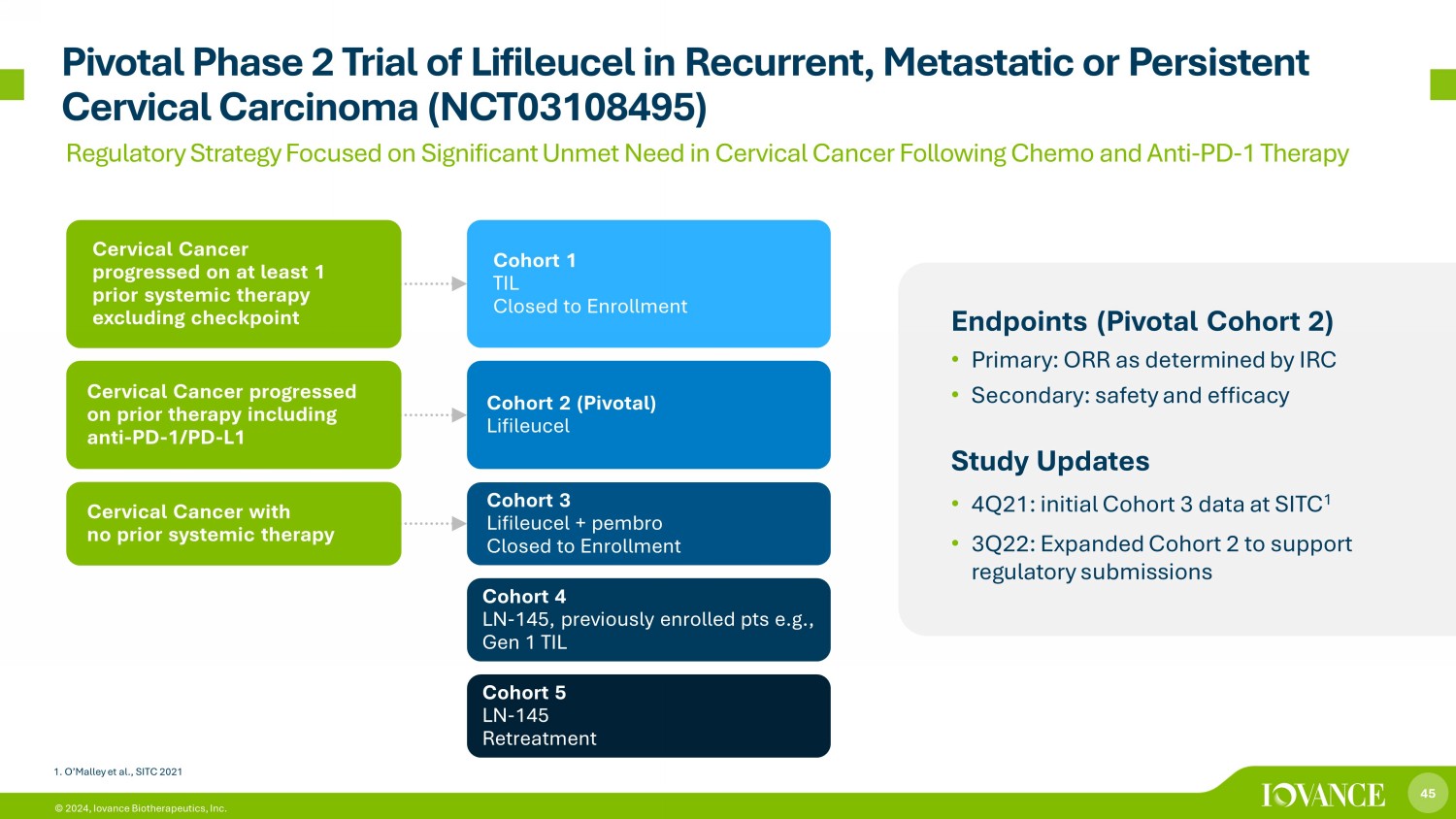
45 © 2024, Iovance Biotherapeutics, Inc. Pivotal Phase 2 Trial of Lifileucel in Recurrent, Metastatic or Persistent Cervical Carcinoma (NCT03108495) Endpoints (Pivotal Cohort 2) • Primary: ORR as determined by IRC • Secondary: safety and efficacy Study Updates • 4Q21: initial Cohort 3 data at SITC 1 • 3Q22: Expanded Cohort 2 to support regulatory submissions Cohort 1 TIL Closed to Enrollment Cohort 2 (Pivotal) Lifileucel Cohort 3 Lifileucel + pembro Closed to Enrollment Cohort 4 LN - 145, previously enrolled pts e.g., Gen 1 TIL Cohort 5 LN - 145 Retreatment Cervical Cancer progressed on at least 1 prior systemic therapy excluding checkpoint Cervical Cancer progressed on prior therapy including anti - PD - 1/PD - L1 Cervical Cancer with no prior systemic therapy 1. O’Malley et al., SITC 2021 Regulatory Strategy Focused on Significant Unmet Need in Cervical Cancer Following Chemo and Anti - PD - 1 Therapy

46 © 2024, Iovance Biotherapeutics, Inc. 46 Next - Generation Research Programs
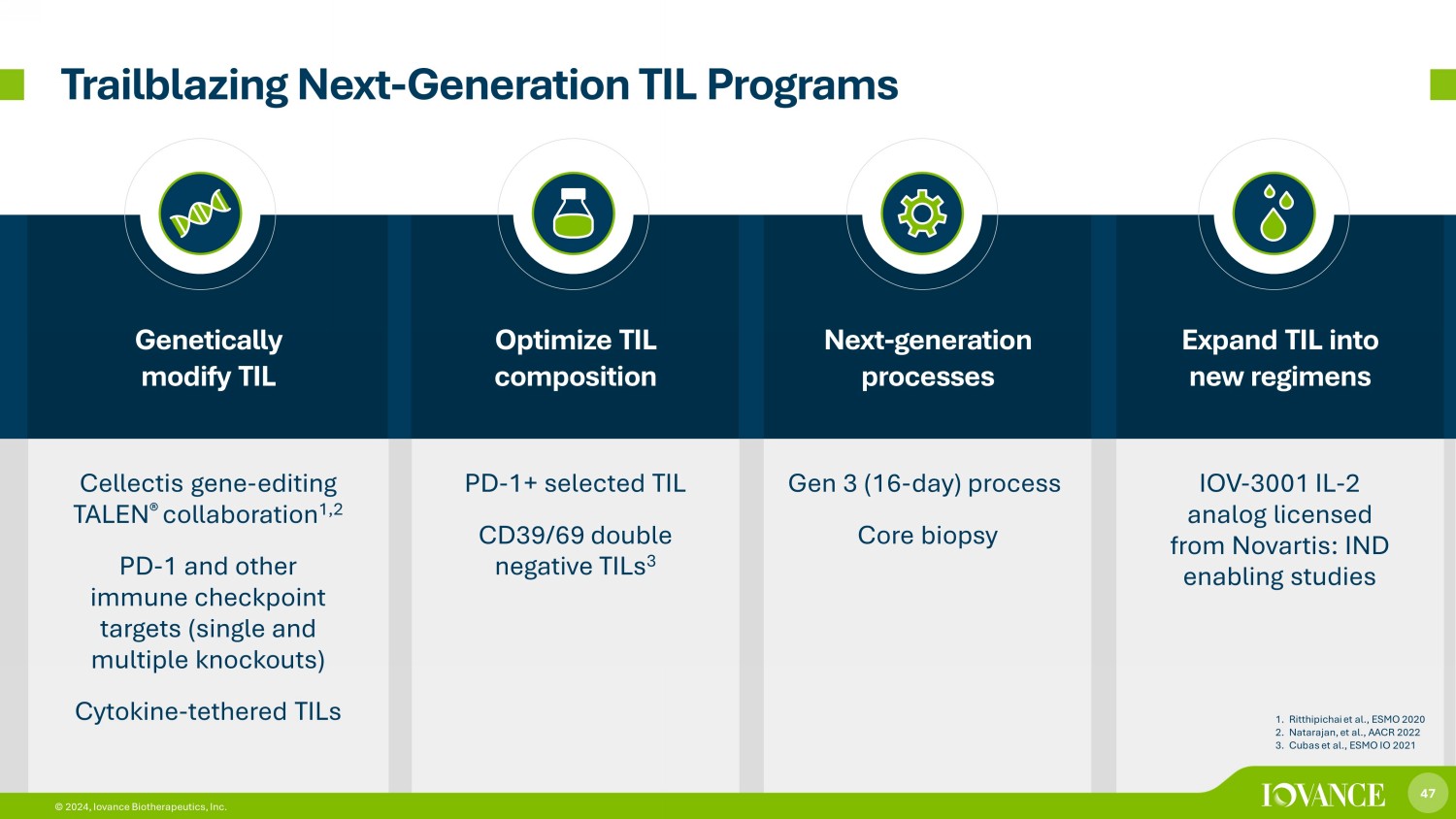
47 © 2024, Iovance Biotherapeutics, Inc. Genetically modify TIL Optimize TIL composition Next - generation processes Expand TIL into new regimens Cellectis gene - editing TALEN ® collaboration 1,2 PD - 1 and other immune checkpoint targets (single and multiple knockouts) Cytokine - tethered TILs PD - 1+ selected TIL CD39/69 double n egative TILs 3 Gen 3 (16 - day) process Core biopsy IOV - 3001 IL - 2 analog licensed from Novartis: IND enabling studies Trailblazing Next - Generation TIL Programs 1. Ritthipichai et al., ESMO 2020 2. Natarajan, et al., AACR 2022 3. Cubas et al., ESMO IO 2021 47 © 2024, Iovance Biotherapeutics, Inc.
48 © 2024, Iovance Biotherapeutics, Inc. 48 Corporate Summary & Milestones
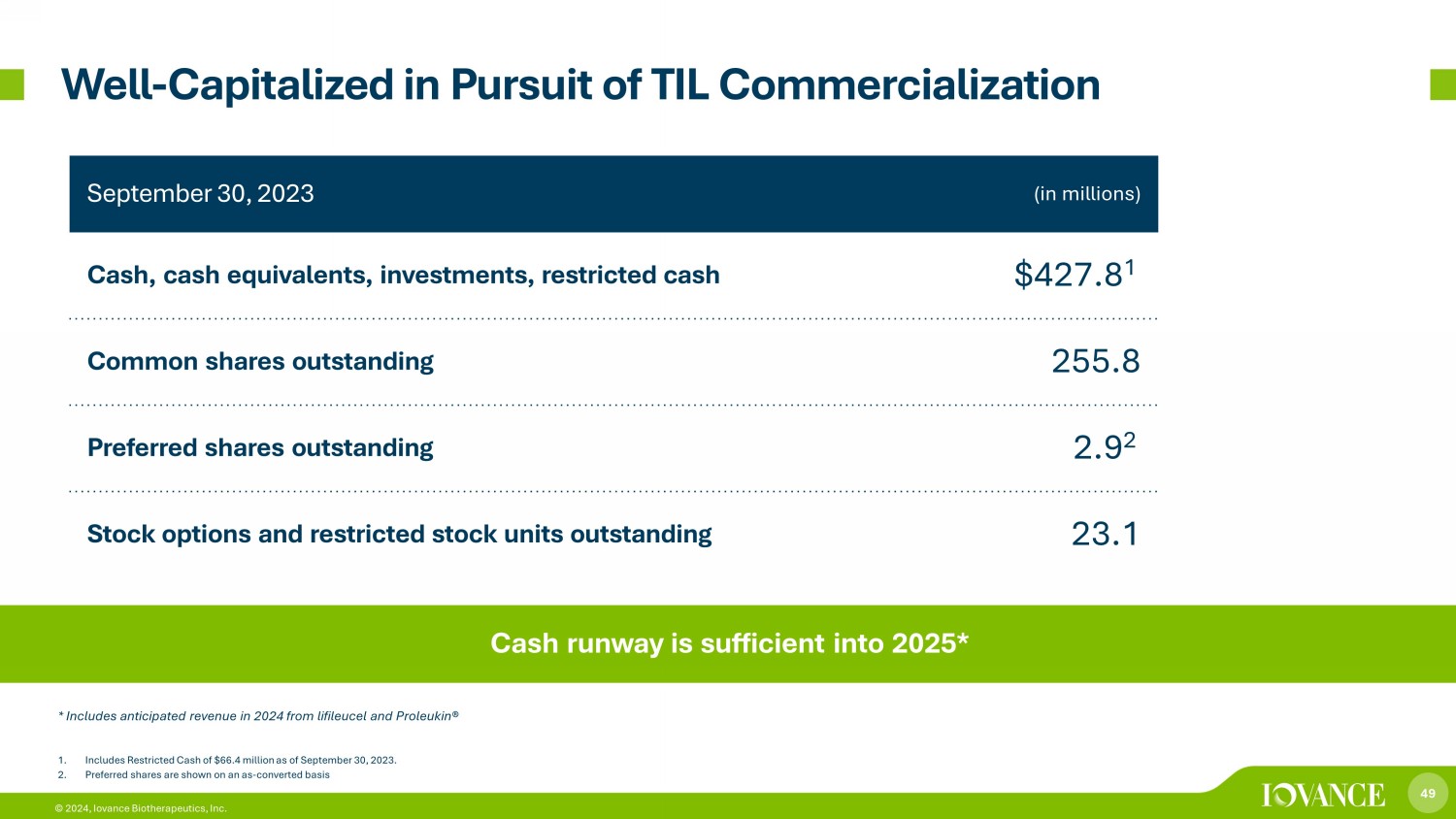
49 © 2024, Iovance Biotherapeutics, Inc. September 30, 2023 (in millions) Cash, cash equivalents, investments, restricted cash $427.8 1 Common shares outstanding 255.8 Preferred shares outstanding 2.9 2 Stock options and restricted stock units outstanding 23.1 1. Includes Restricted Cash of $66.4 million as of September 30, 2023. 2. Preferred shares are shown on an as - converted basis Well - Capitalized in Pursuit of TIL Commercialization Cash runway is sufficient into 2025* * Includes anticipated revenue in 2024 from lifileucel and Proleukin®

50 © 2024, Iovance Biotherapeutics, Inc. Broad, Iovance - Owned IP Around TIL Therapy TIL products and compositions: Gen 2, Gen 3, use of co - stimulants, selection of TIL, stable and transient genetic modifications, cryopreservation 1 Tumor Sample Procurement 3 4 NMA - LD TIL Infusion 5 IL - 2 Infusions 4 2 TIL from: • Tumor • Marrow infiltrating lymphocytes • Peripheral blood lymphocytes • Frozen tumor technologies • Remnant TIL and digest processes • Combination of TIL and ICIs including PD - 1 antibodies • Patient subpopulations IL - 2 variants and regimens x 60+ granted or allowed US and international patents x Compositions of matter for TIL products x Methods of treatment in a broad range of cancers x Manufacturing processes
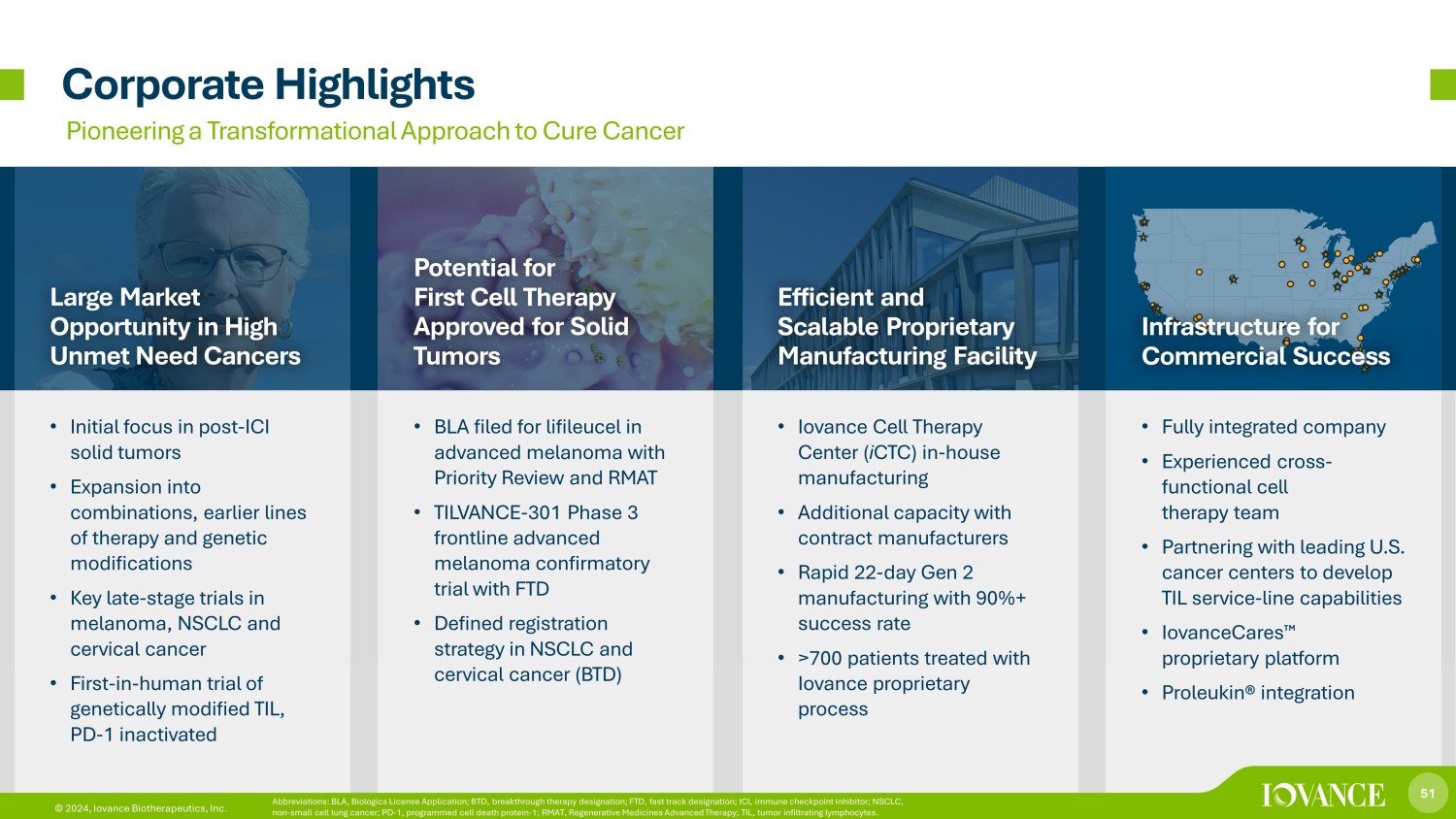
51 © 2024, Iovance Biotherapeutics, Inc. Corporate Highlights Pioneering a Transformational Approach to Cure Cancer Large Market Opportunity in High Unmet Need Cancers Potential for First Cell Therapy Approved for Solid Tumors Efficient and Scalable Proprietary Manufacturing Facility Infrastructure for Commercial Success • Initial focus in post - ICI solid tumors • Expansion into combinations, earlier lines of therapy and genetic modifications • Key late - stage trials in melanoma, NSCLC and cervical cancer • First - in - human trial of genetically modified TIL, PD - 1 inactivated • BLA filed for lifileucel in advanced melanoma with Priority Review and RMAT • TILVANCE - 301 Phase 3 frontline advanced melanoma confirmatory trial with FTD • Defined registration strategy in NSCLC and cervical cancer (BTD) • Iovance Cell Therapy Center ( i CTC) in - house manufacturing • Additional capacity with contract manufacturers • Rapid 22 - day Gen 2 manufacturing with 90%+ success rate • >700 patients treated with Iovance proprietary process • Fully integrated company • Experienced cross - functional cell therapy team • Partnering with leading U.S. cancer centers to develop TIL service - line capabilities • IovanceCares ¯ proprietary platform • Proleukin® integration 51 © 2024, Iovance Biotherapeutics, Inc. Abbreviations: BLA, Biologics License Application; BTD, breakthrough therapy designation; FTD, fast track designation; ICI, i mmu ne checkpoint inhibitor; NSCLC, non - small cell lung cancer; PD - 1, programmed cell death protein - 1; RMAT, Regenerative Medicines Advanced Therapy; TIL, tumor inf iltrating lymphocytes.
52 © 2024, Iovance Biotherapeutics, Inc. REGULATORY □ BLA: Complete rolling BLA submission for lifileucel in post - anti - PD - 1 advanced melanoma in Q1 2023; late cycle meeting completed and BLA on track toward PDUFA date □ Ex - U.S. regulatory submissions: Initiate preparation of submissions in ex - U.S. markets PIPELINE □ Melanoma: enroll patients in frontline advanced melanoma Phase 3 confirmatory trial □ NSCLC: report data and continue to enroll IOV - LUN - 202, IOV - COM - 202, IOV - GM1 - 201 trials □ Cervical: enroll additional patients in registrational Cohort 2 □ Research: advance new products toward clinic, including additional genetically - modified TIL therapies MANUFACTURING □ Execute GMP commercial readiness activities to support BLA approval including passing PLI inspections □ Supply lifileucel at launch: Ramped up iCTC and CDMO capacity in preparation for launch COMMERCIAL □ Prepare for commercial launch □ Close transaction and successfully integrate Proleukin® business 2023 Milestones
53 © 2024, Iovance Biotherapeutics, Inc. REGULATORY □ Obtain FDA approval for lifileucel in advanced melanoma (PDUFA date: February 24, 2024) □ Submit EMA regulatory submission in 1 st half of 2024 □ Submit additional ex - US submissions in 2 nd half of 2024 □ Meet with FDA to discuss NSCLC registrational path/frontline study PIPELINE □ Report clinical and pre - clinical data □ Resume enrollment in IOV - LUN - 202 □ Initiate Phase 2 trial in endometrial cancer □ Continue to enroll patients in clinical trials for advanced melanoma, NSCLC and gynecological cancers □ Advance new products toward clinic, including additional genetically - modified TIL therapies MANUFACTURING □ Fulfill patient demand for commercial launch and clinical trials □ Further expand capacity to meet US and ex - US demand COMMERCIAL □ Execute commercial launch (1Q24) □ On - board 50 ATCs within 90 days of PDUFA date Anticipated 2024 Milestones

54 © 2024, Iovance Biotherapeutics, Inc. © 2024, Iovance Biotherapeutics, Inc. Thank You
v3.23.4
Cover
|
Jan. 08, 2024 |
| Cover [Abstract] |
|
| Document Type |
8-K
|
| Amendment Flag |
false
|
| Document Period End Date |
Jan. 08, 2024
|
| Entity File Number |
001-36860
|
| Entity Registrant Name |
IOVANCE BIOTHERAPEUTICS, INC.
|
| Entity Central Index Key |
0001425205
|
| Entity Tax Identification Number |
75-3254381
|
| Entity Incorporation, State or Country Code |
DE
|
| Entity Address, Address Line One |
825
Industrial Road
|
| Entity Address, Address Line Two |
Suite 400
|
| Entity Address, City or Town |
San Carlos
|
| Entity Address, State or Province |
CA
|
| Entity Address, Postal Zip Code |
94070
|
| City Area Code |
650
|
| Local Phone Number |
260-7120
|
| Written Communications |
false
|
| Soliciting Material |
false
|
| Pre-commencement Tender Offer |
false
|
| Pre-commencement Issuer Tender Offer |
false
|
| Title of 12(b) Security |
Common stock, par value $0.000041666 per value
|
| Trading Symbol |
IOVA
|
| Security Exchange Name |
NASDAQ
|
| Entity Emerging Growth Company |
false
|
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Iovance Biotherapeutics (NASDAQ:IOVA)
과거 데이터 주식 차트
부터 4월(4) 2024 으로 5월(5) 2024

Iovance Biotherapeutics (NASDAQ:IOVA)
과거 데이터 주식 차트
부터 5월(5) 2023 으로 5월(5) 2024
